{"title":"基于机器学习的主动脉夹层院内死亡率预后模型:从重症监护医学的角度看问题。","authors":"Jiahao Lei, Zhuojing Zhang, Yixuan Li, Zhaoyu Wu, Hongji Pu, Zhijue Xu, Xinrui Yang, Jiateng Hu, Guang Liu, Peng Qiu, Tao Chen, Xinwu Lu","doi":"10.1177/20552076241269450","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Aortic dissection (AD) is a severe emergency with high morbidity and mortality, necessitating strict monitoring and management. This retrospective study aimed to identify prognostic factors and establish predictive models for in-hospital mortality among AD patients in the intensive care unit (ICU).</p><p><strong>Methods: </strong>We retrieved ICU admission records of AD patients from the Medical Information Mart for Intensive Care (MIMIC)-IV critical care data set and the eICU Collaborative Research Database. Functional data analysis was further applied to estimate continuous vital sign processes, and variables associated with in-hospital mortality were identified through univariate analyses. Subsequently, we employed multivariable logistic regression and machine learning techniques, including simple decision tree, random forest (RF), and eXtreme Gradient Boosting (XGBoost) to develop prognostic models for in-hospital mortality.</p><p><strong>Results: </strong>Given 643 ICU admissions from MIMIC-IV and 501 admissions from eICU, 29 and 28 prognostic factors were identified from each database through univariate analyses, respectively. For prognostic model construction, 507 MIMIC-IV admissions were divided into 406 (80%) for training and 101 (20%) for internal validation, and 87 eICU admissions were included as an external validation group. Of the four models tested, the RF consistently exhibited the best performance among different variable subsets, boasting area under the receiver operating characteristic curves of 0.870 and 0.850. The models highlighted the mean 24-h fluid intake as the most potent prognostic factor.</p><p><strong>Conclusions: </strong>The current prognostic models effectively forecasted in-hospital mortality among AD patients, and they pinpointed noteworthy prognostic factors, including initial blood pressure upon ICU admission and mean 24-h fluid intake.</p>","PeriodicalId":51333,"journal":{"name":"DIGITAL HEALTH","volume":"10 ","pages":"20552076241269450"},"PeriodicalIF":3.3000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11334245/pdf/","citationCount":"0","resultStr":"{\"title\":\"Machine learning-based prognostic model for in-hospital mortality of aortic dissection: Insights from an intensive care medicine perspective.\",\"authors\":\"Jiahao Lei, Zhuojing Zhang, Yixuan Li, Zhaoyu Wu, Hongji Pu, Zhijue Xu, Xinrui Yang, Jiateng Hu, Guang Liu, Peng Qiu, Tao Chen, Xinwu Lu\",\"doi\":\"10.1177/20552076241269450\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Aortic dissection (AD) is a severe emergency with high morbidity and mortality, necessitating strict monitoring and management. This retrospective study aimed to identify prognostic factors and establish predictive models for in-hospital mortality among AD patients in the intensive care unit (ICU).</p><p><strong>Methods: </strong>We retrieved ICU admission records of AD patients from the Medical Information Mart for Intensive Care (MIMIC)-IV critical care data set and the eICU Collaborative Research Database. Functional data analysis was further applied to estimate continuous vital sign processes, and variables associated with in-hospital mortality were identified through univariate analyses. Subsequently, we employed multivariable logistic regression and machine learning techniques, including simple decision tree, random forest (RF), and eXtreme Gradient Boosting (XGBoost) to develop prognostic models for in-hospital mortality.</p><p><strong>Results: </strong>Given 643 ICU admissions from MIMIC-IV and 501 admissions from eICU, 29 and 28 prognostic factors were identified from each database through univariate analyses, respectively. For prognostic model construction, 507 MIMIC-IV admissions were divided into 406 (80%) for training and 101 (20%) for internal validation, and 87 eICU admissions were included as an external validation group. Of the four models tested, the RF consistently exhibited the best performance among different variable subsets, boasting area under the receiver operating characteristic curves of 0.870 and 0.850. The models highlighted the mean 24-h fluid intake as the most potent prognostic factor.</p><p><strong>Conclusions: </strong>The current prognostic models effectively forecasted in-hospital mortality among AD patients, and they pinpointed noteworthy prognostic factors, including initial blood pressure upon ICU admission and mean 24-h fluid intake.</p>\",\"PeriodicalId\":51333,\"journal\":{\"name\":\"DIGITAL HEALTH\",\"volume\":\"10 \",\"pages\":\"20552076241269450\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11334245/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"DIGITAL HEALTH\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20552076241269450\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"DIGITAL HEALTH","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20552076241269450","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Machine learning-based prognostic model for in-hospital mortality of aortic dissection: Insights from an intensive care medicine perspective.
Objective: Aortic dissection (AD) is a severe emergency with high morbidity and mortality, necessitating strict monitoring and management. This retrospective study aimed to identify prognostic factors and establish predictive models for in-hospital mortality among AD patients in the intensive care unit (ICU).
Methods: We retrieved ICU admission records of AD patients from the Medical Information Mart for Intensive Care (MIMIC)-IV critical care data set and the eICU Collaborative Research Database. Functional data analysis was further applied to estimate continuous vital sign processes, and variables associated with in-hospital mortality were identified through univariate analyses. Subsequently, we employed multivariable logistic regression and machine learning techniques, including simple decision tree, random forest (RF), and eXtreme Gradient Boosting (XGBoost) to develop prognostic models for in-hospital mortality.
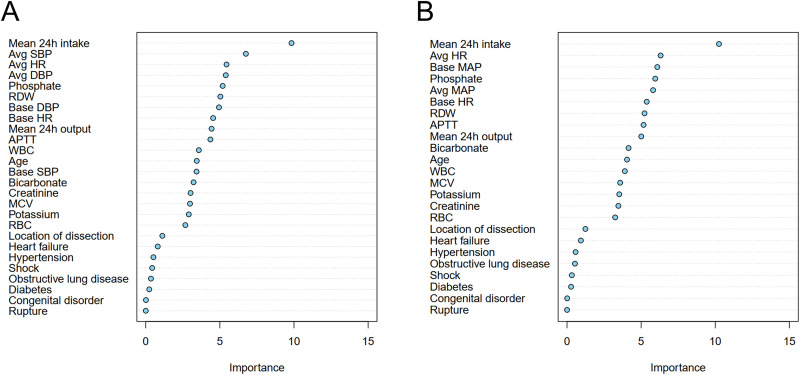
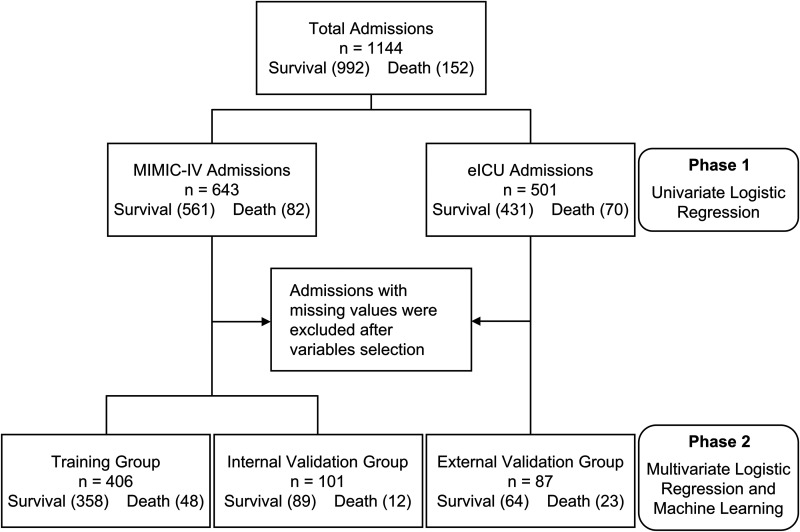
Results: Given 643 ICU admissions from MIMIC-IV and 501 admissions from eICU, 29 and 28 prognostic factors were identified from each database through univariate analyses, respectively. For prognostic model construction, 507 MIMIC-IV admissions were divided into 406 (80%) for training and 101 (20%) for internal validation, and 87 eICU admissions were included as an external validation group. Of the four models tested, the RF consistently exhibited the best performance among different variable subsets, boasting area under the receiver operating characteristic curves of 0.870 and 0.850. The models highlighted the mean 24-h fluid intake as the most potent prognostic factor.
Conclusions: The current prognostic models effectively forecasted in-hospital mortality among AD patients, and they pinpointed noteworthy prognostic factors, including initial blood pressure upon ICU admission and mean 24-h fluid intake.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


