Marcus Westerberg , Hans Garmo , David Robinson , Pär Stattin , Rolf Gedeborg
{"title":"使用新的合并症指数进行目标试验模拟,可提供与随机试验相当的风险估计值。","authors":"Marcus Westerberg , Hans Garmo , David Robinson , Pär Stattin , Rolf Gedeborg","doi":"10.1016/j.jclinepi.2024.111504","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>To quantify the ability of two new comorbidity indices to adjust for confounding, by benchmarking a target trial emulation against the randomized controlled trial (RCT) result.</p></div><div><h3>Study Design and Setting</h3><p>Observational study including 18,316 men from Prostate Cancer data Base Sweden 5.0, diagnosed with prostate cancer between 2008 and 2019 and treated with primary radical prostatectomy (RP, <em>n</em> = 14,379) or radiotherapy (RT, <em>n</em> = 3,937). The effect on adjusted risk of death from any cause after adjustment for comorbidity by use of two new comorbidity indices, the multidimensional diagnosis-based comorbidity index and the drug comorbidity index, were compared to adjustment for the Charlson comorbidity index (CCI).</p></div><div><h3>Results</h3><p>Risk of death was higher after RT than RP (hazard ratio [HR] = 1.94; 95% confidence interval [CI]: 1.70–2.21). The difference decreased when adjusting for age, cancer characteristics, and CCI (HR = 1.32, 95% CI: 1.06–1.66). Adjustment for the two new comorbidity indices further attenuated the difference (HR 1.14, 95% CI 0.91–1.44). Emulation of a hypothetical pragmatic trial where also older men with any type of baseline comorbidity were included, largely confirmed these results (HR 1.10; 95% CI 0.95–1.26).</p></div><div><h3>Conclusion</h3><p>Adjustment for comorbidity using two new indices provided comparable risk of death from any cause in line with results of a RCT. Similar results were seen in a broader study population, more representative of clinical practice.</p></div>","PeriodicalId":51079,"journal":{"name":"Journal of Clinical Epidemiology","volume":"174 ","pages":"Article 111504"},"PeriodicalIF":7.3000,"publicationDate":"2024-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0895435624002609/pdfft?md5=66bdbf3013b9d88ca0da75aec3fcdb62&pid=1-s2.0-S0895435624002609-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Target trial emulation using new comorbidity indices provided risk estimates comparable to a randomized trial\",\"authors\":\"Marcus Westerberg , Hans Garmo , David Robinson , Pär Stattin , Rolf Gedeborg\",\"doi\":\"10.1016/j.jclinepi.2024.111504\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><p>To quantify the ability of two new comorbidity indices to adjust for confounding, by benchmarking a target trial emulation against the randomized controlled trial (RCT) result.</p></div><div><h3>Study Design and Setting</h3><p>Observational study including 18,316 men from Prostate Cancer data Base Sweden 5.0, diagnosed with prostate cancer between 2008 and 2019 and treated with primary radical prostatectomy (RP, <em>n</em> = 14,379) or radiotherapy (RT, <em>n</em> = 3,937). The effect on adjusted risk of death from any cause after adjustment for comorbidity by use of two new comorbidity indices, the multidimensional diagnosis-based comorbidity index and the drug comorbidity index, were compared to adjustment for the Charlson comorbidity index (CCI).</p></div><div><h3>Results</h3><p>Risk of death was higher after RT than RP (hazard ratio [HR] = 1.94; 95% confidence interval [CI]: 1.70–2.21). The difference decreased when adjusting for age, cancer characteristics, and CCI (HR = 1.32, 95% CI: 1.06–1.66). Adjustment for the two new comorbidity indices further attenuated the difference (HR 1.14, 95% CI 0.91–1.44). Emulation of a hypothetical pragmatic trial where also older men with any type of baseline comorbidity were included, largely confirmed these results (HR 1.10; 95% CI 0.95–1.26).</p></div><div><h3>Conclusion</h3><p>Adjustment for comorbidity using two new indices provided comparable risk of death from any cause in line with results of a RCT. Similar results were seen in a broader study population, more representative of clinical practice.</p></div>\",\"PeriodicalId\":51079,\"journal\":{\"name\":\"Journal of Clinical Epidemiology\",\"volume\":\"174 \",\"pages\":\"Article 111504\"},\"PeriodicalIF\":7.3000,\"publicationDate\":\"2024-08-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0895435624002609/pdfft?md5=66bdbf3013b9d88ca0da75aec3fcdb62&pid=1-s2.0-S0895435624002609-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0895435624002609\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0895435624002609","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
目的:通过将目标试验模拟与随机对照试验结果进行对比,量化两种新的合并症指数调整混杂因素的能力:通过将目标试验模拟与随机对照试验结果进行比对,量化两种新合并症指数调整混杂因素的能力:观察性研究包括瑞典前列腺癌数据库5.0中的18 316名男性,他们在2008年至2019年间被诊断为前列腺癌,并接受了原发性根治性前列腺切除术(n=14 379)或放射治疗(n=3937)。通过使用两种新的合并症指数(基于诊断的多维合并症指数(MDCI)和药物合并症指数(DCI))对合并症进行调整后,调整后的任何原因死亡风险对调整后的死亡风险的影响与夏尔森合并症指数(CCI)的影响进行了比较:结果:放疗后的死亡风险高于根治性前列腺切除术(HR=1.94;95% CI:1.70 - 2.21)。调整年龄、癌症特征和 CCI 后,差异有所缩小(HR=1.32;95% CI:1.06 - 1.66)。调整两个新的合并症指数后,差异进一步缩小(HR 1.14,95% CI 0.91 - 1.44)。在一项假定的实用性试验中,也纳入了有任何基线合并症的老年男性,该试验在很大程度上证实了这些结果(HR 1.10; 95% CI 0.95 - 1.26):结论:使用两种新指数对合并症进行调整后,任何原因导致的死亡风险都具有可比性,这与随机对照试验的结果一致。类似的结果也出现在更广泛的研究人群中,更能代表临床实践。
Target trial emulation using new comorbidity indices provided risk estimates comparable to a randomized trial
Objectives
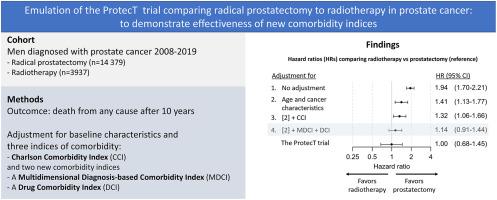
To quantify the ability of two new comorbidity indices to adjust for confounding, by benchmarking a target trial emulation against the randomized controlled trial (RCT) result.
Study Design and Setting
Observational study including 18,316 men from Prostate Cancer data Base Sweden 5.0, diagnosed with prostate cancer between 2008 and 2019 and treated with primary radical prostatectomy (RP, n = 14,379) or radiotherapy (RT, n = 3,937). The effect on adjusted risk of death from any cause after adjustment for comorbidity by use of two new comorbidity indices, the multidimensional diagnosis-based comorbidity index and the drug comorbidity index, were compared to adjustment for the Charlson comorbidity index (CCI).
Results
Risk of death was higher after RT than RP (hazard ratio [HR] = 1.94; 95% confidence interval [CI]: 1.70–2.21). The difference decreased when adjusting for age, cancer characteristics, and CCI (HR = 1.32, 95% CI: 1.06–1.66). Adjustment for the two new comorbidity indices further attenuated the difference (HR 1.14, 95% CI 0.91–1.44). Emulation of a hypothetical pragmatic trial where also older men with any type of baseline comorbidity were included, largely confirmed these results (HR 1.10; 95% CI 0.95–1.26).
Conclusion
Adjustment for comorbidity using two new indices provided comparable risk of death from any cause in line with results of a RCT. Similar results were seen in a broader study population, more representative of clinical practice.
期刊介绍:
The Journal of Clinical Epidemiology strives to enhance the quality of clinical and patient-oriented healthcare research by advancing and applying innovative methods in conducting, presenting, synthesizing, disseminating, and translating research results into optimal clinical practice. Special emphasis is placed on training new generations of scientists and clinical practice leaders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


