{"title":"病例报告:慢性肾病贫血患者罗沙司他用药过量:超越微不足道后果的洞察力。","authors":"Long-Guang Zhang, Xue-Juan Ma, Xiang-Yang Li","doi":"10.3389/fneph.2024.1413496","DOIUrl":null,"url":null,"abstract":"<p><p>A 71-year-old man with a 20-year history of grade 3 hypertension experienced kidney dysfunction 2 years earlier. His serum creatinine (SCr) at the time was 140 μmol/L [with estimated glomerular filtration rate (eGFR) of 43.9 ml/min per 1.73m<sup>2</sup>], for which he received irbesartan since. At initial presentation, the spot urine dipstick protein was 1+, with an albumin-to-creatinine ratio of 230 mg/g (0-30) and normal urine sediments. The SCr was 176 μmol/L (eGFR = 32.8 ml/min per 1.73m<sup>2</sup>). The hemoglobulin (Hb) level decreased from 102 to 96 g/L despite oral ferrous succinate 100 mg twice daily starting 2 months ago. Roxadustat (ROXA) 50 mg (body weight, 70 kg) three times weekly was then prescribed. Unfortunately, the patient mistakenly took the drug at 50 mg three times a day (i.e., 1,050 mg instead of the intended 150 mg per week), which was 3.5 times the recommended starting dose for non-dialysis-dependent chronic kidney disease (CKD) patients (100 mg three times weekly for body weight >60 kg) and two times the highest drug manual-recommended weekly dose (2.5 mg/kg three times weekly) approved in the country. When the attending nephrologist discovered the misuse 1 month later, the patient reported no apparent discomfort, and his home blood pressure was in the range 110-130/60-80 mmHg. Repeat blood tests showed that the Hb increased from 96 to 163 g/L and the SCr from 199 to 201 μmol/L in a month. The serum alanine transaminase (ALT) remained within the normal range (from 12 U/L at baseline to 20 U/L), while the serum total and indirect bilirubin levels were slightly elevated. ROXA was withheld immediately. In 30 days, the serum bilirubin returned to baseline, but the Hb decreased from 163 to 140 g/L, and then to 108 g/L after 3 months. On the other hand, the SCr increased from 179 to 203 μmol/L. At 9 months after the initial dosing, when the SCr increased to 256 μmol/L and the Hb decreased to 94 g/L again, ROXA 50 mg three times weekly was reinitiated uneventfully. Herein, by introducing a case who erroneously consumed twice the highest recommended dose of ROXA for a month, but had apparently no obvious discomfort or unfavorable consequence, we attempt to provide a brief overview of the mechanism of action, characteristics, drug metabolism, and side effect profile associated with this agent.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"4 ","pages":"1413496"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11327132/pdf/","citationCount":"0","resultStr":"{\"title\":\"Case report: Roxadustat overdose in an anemia patient of chronic kidney disease: insight beyond insignificant consequence.\",\"authors\":\"Long-Guang Zhang, Xue-Juan Ma, Xiang-Yang Li\",\"doi\":\"10.3389/fneph.2024.1413496\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 71-year-old man with a 20-year history of grade 3 hypertension experienced kidney dysfunction 2 years earlier. His serum creatinine (SCr) at the time was 140 μmol/L [with estimated glomerular filtration rate (eGFR) of 43.9 ml/min per 1.73m<sup>2</sup>], for which he received irbesartan since. At initial presentation, the spot urine dipstick protein was 1+, with an albumin-to-creatinine ratio of 230 mg/g (0-30) and normal urine sediments. The SCr was 176 μmol/L (eGFR = 32.8 ml/min per 1.73m<sup>2</sup>). The hemoglobulin (Hb) level decreased from 102 to 96 g/L despite oral ferrous succinate 100 mg twice daily starting 2 months ago. Roxadustat (ROXA) 50 mg (body weight, 70 kg) three times weekly was then prescribed. Unfortunately, the patient mistakenly took the drug at 50 mg three times a day (i.e., 1,050 mg instead of the intended 150 mg per week), which was 3.5 times the recommended starting dose for non-dialysis-dependent chronic kidney disease (CKD) patients (100 mg three times weekly for body weight >60 kg) and two times the highest drug manual-recommended weekly dose (2.5 mg/kg three times weekly) approved in the country. When the attending nephrologist discovered the misuse 1 month later, the patient reported no apparent discomfort, and his home blood pressure was in the range 110-130/60-80 mmHg. Repeat blood tests showed that the Hb increased from 96 to 163 g/L and the SCr from 199 to 201 μmol/L in a month. The serum alanine transaminase (ALT) remained within the normal range (from 12 U/L at baseline to 20 U/L), while the serum total and indirect bilirubin levels were slightly elevated. ROXA was withheld immediately. In 30 days, the serum bilirubin returned to baseline, but the Hb decreased from 163 to 140 g/L, and then to 108 g/L after 3 months. On the other hand, the SCr increased from 179 to 203 μmol/L. At 9 months after the initial dosing, when the SCr increased to 256 μmol/L and the Hb decreased to 94 g/L again, ROXA 50 mg three times weekly was reinitiated uneventfully. Herein, by introducing a case who erroneously consumed twice the highest recommended dose of ROXA for a month, but had apparently no obvious discomfort or unfavorable consequence, we attempt to provide a brief overview of the mechanism of action, characteristics, drug metabolism, and side effect profile associated with this agent.</p>\",\"PeriodicalId\":73091,\"journal\":{\"name\":\"Frontiers in nephrology\",\"volume\":\"4 \",\"pages\":\"1413496\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11327132/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fneph.2024.1413496\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2024.1413496","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Case report: Roxadustat overdose in an anemia patient of chronic kidney disease: insight beyond insignificant consequence.
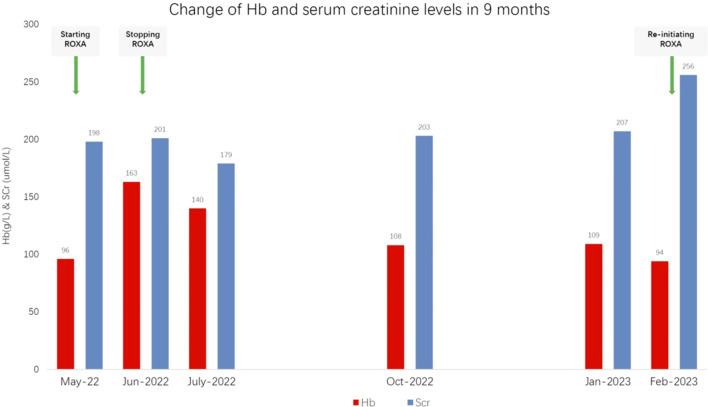
A 71-year-old man with a 20-year history of grade 3 hypertension experienced kidney dysfunction 2 years earlier. His serum creatinine (SCr) at the time was 140 μmol/L [with estimated glomerular filtration rate (eGFR) of 43.9 ml/min per 1.73m2], for which he received irbesartan since. At initial presentation, the spot urine dipstick protein was 1+, with an albumin-to-creatinine ratio of 230 mg/g (0-30) and normal urine sediments. The SCr was 176 μmol/L (eGFR = 32.8 ml/min per 1.73m2). The hemoglobulin (Hb) level decreased from 102 to 96 g/L despite oral ferrous succinate 100 mg twice daily starting 2 months ago. Roxadustat (ROXA) 50 mg (body weight, 70 kg) three times weekly was then prescribed. Unfortunately, the patient mistakenly took the drug at 50 mg three times a day (i.e., 1,050 mg instead of the intended 150 mg per week), which was 3.5 times the recommended starting dose for non-dialysis-dependent chronic kidney disease (CKD) patients (100 mg three times weekly for body weight >60 kg) and two times the highest drug manual-recommended weekly dose (2.5 mg/kg three times weekly) approved in the country. When the attending nephrologist discovered the misuse 1 month later, the patient reported no apparent discomfort, and his home blood pressure was in the range 110-130/60-80 mmHg. Repeat blood tests showed that the Hb increased from 96 to 163 g/L and the SCr from 199 to 201 μmol/L in a month. The serum alanine transaminase (ALT) remained within the normal range (from 12 U/L at baseline to 20 U/L), while the serum total and indirect bilirubin levels were slightly elevated. ROXA was withheld immediately. In 30 days, the serum bilirubin returned to baseline, but the Hb decreased from 163 to 140 g/L, and then to 108 g/L after 3 months. On the other hand, the SCr increased from 179 to 203 μmol/L. At 9 months after the initial dosing, when the SCr increased to 256 μmol/L and the Hb decreased to 94 g/L again, ROXA 50 mg three times weekly was reinitiated uneventfully. Herein, by introducing a case who erroneously consumed twice the highest recommended dose of ROXA for a month, but had apparently no obvious discomfort or unfavorable consequence, we attempt to provide a brief overview of the mechanism of action, characteristics, drug metabolism, and side effect profile associated with this agent.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


