Abdullah N. M. Alqahtani, Sandrine Jayne, Matthew J. Ahearne, Christopher S. Trethewey, Sai S. Duraisingham, Susann Lehmann, Caroline M. Cowley, Martin J. S. Dyer, Harriet S. Walter
{"title":"监测复发/难治套细胞淋巴瘤特殊应答者队列中对替瑞布替尼的分子反应","authors":"Abdullah N. M. Alqahtani, Sandrine Jayne, Matthew J. Ahearne, Christopher S. Trethewey, Sai S. Duraisingham, Susann Lehmann, Caroline M. Cowley, Martin J. S. Dyer, Harriet S. Walter","doi":"10.1002/jha2.966","DOIUrl":null,"url":null,"abstract":"<p>To the Editor,</p><p>Inhibitors of Bruton's tyrosine kinase (BTK) in chronic lymphocytic leukemia (CLL) result in durable responses in nearly all patients [<span>1</span>]. In contrast, in more aggressive B-cell malignancies, including diffuse large B cell lymphoma (DLBCL) and mantle cell lymphoma (MCL), responses to single agent BTK inhibitors (BTKi) occur only in subsets of patients and are mostly of brief duration. However, exceptional responses may occur [<span>2-6</span>].</p><p>In relapsed/refractory (R/R) MCL, median progression-free survival (PFS) with single-agent covalent BTKi range from 12 (ibrutinib) to 20 months (acalabrutinib ACE-LY-004 NCT02213926 study) (Table S1) [<span>7-9</span>]. Analysis of responding patients in ACE-LY-004 showed that 8/29 evaluable patients eradicated minimal residual disease (MRD) using the quantitative ClonoSEQ next-generation sequencing assay of cellular peripheral blood DNA [<span>10</span>]. However, molecular determinants of responsiveness to BTKi in MCL, and clinical significance of attaining MRD negativity in this setting remain unknown.</p><p>Like acalabrutinib, tirabrutinib is a highly selective BTKi, binding covalently to BTKC481 via a reactive acyl alkyne group. Although only 16 MCL patients were treated with single-agent tirabrutinib within the POE001 phase 1 trial (NCT01659255), extended follow-up showed an estimated median PFS of 25.8 months at 3 years [<span>11</span>]. Three patients from this cohort, described below, attained complete responses lasting over 72 months, despite adverse prognostic features at diagnosis including <i>TP53</i> mutations, blastoid morphology, and refractoriness to immunochemotherapy. In these exceptional responders [<span>12</span>], we sought to determine common features or a tumoral mutational signature that might predict exceptional responsiveness. Secondly, we determined the depth of response using digital droplet PCR (ddPCR) in both plasma and cellular DNA samples and whether serial assessment of levels of cellular and plasma circulating tumor (ct) DNA samples might presage relapse.</p><p>Clinical and laboratory details of the three cases are given in Table 1. A schema of the treatment timelines is shown in Figure 1. Full materials and methods are found in the Supporting Information. The three patients (201-139, 201-162, and 201-170) were all treated at our center and received either 480 or 600 mg of tirabrutinib once per day. All entered a clinical and radiological remission. One patient (patient 201-162) with primary immunochemotherapy-refractory disease remains in complete remission (CR) > 108 months from trial initiation. However, in 2020, they developed estrogen receptor positive grade 2 invasive ductal breast cancer, necessitating temporary discontinuation of tirabrutinib for 4 months. The breast cancer was treated radically with surgical resection, post operative radiotherapy and tamoxifen. There remains no clinical or radiological evidence of recurrence. The other two patients relapsed 91 and 72 months after initiating tirabrutinib. Due to comorbidities, no further therapy was attempted in patient 201-170 and the patient died rapidly from uncontrolled disease. Patient 201-139 received rituximab, bendamustine, cytosine arabinoside, and subsequently pirtobrutinib with the aim of proceeding to chimeric antigen receptor (CAR)-T cell therapy, but failed to respond adequately.</p><p>Whole exome sequencing showed t(11;14)(q13;q32) with breakpoints in <i>CCND1</i> and <i>IGH</i> as anticipated, but there were no other common mutations (Table S2). Two patients exhibited <i>TP53</i> mutation (pL194R and pR181H), one <i>KMT2D</i> mutation (p.S2773Lfs*72), and one patient had two <i>ATM</i> mutations. All three cases showed unmutated (> 99% homology to germline) <i>IGHV</i> gene segment usage; two cases utilized <i>IGHV4-34</i>, the other <i>IGHV3-23</i>. Unmutated <i>IGHV4-34</i> is seen in 15% of MCL and in 15% of the non-germinal center subtype of DLBCL, including the MCD subgroup, sensitive to BTKi. Unmutated IGHV4-34 recognizes autoantigens on the surface of malignant B cells, shown to result in chronic active BCR signaling in activated B-cell-like DLBCL models [<span>13</span>]. At relapse, in patient 201-139 mutations in <i>PLCG2</i> (p.M1141T, 54% VAF), previously described in relapsed CLL with ibrutinib, and in <i>NFKB2</i> (p.G373_G374insEGVLC, 36% VAF) that activates the alternative nuclear factor κappa B pathway were seen. No <i>BTK</i> mutations were present, supporting prior findings [<span>14</span>].</p><p>Interestingly, in all 3 cases, we observed a complete absence of peripheral blood CD19+ B cells with tirabrutinib, consistent with B cell aplasia. In one case (201-139) bone marrow analysis confirmed a B-cell differentiation block at the CD19+ CD38+ sIg- B-cell precursor stage (Figure S1A). In this patient, B cell aplasia resulted in hypogammaglobulinemia and recurrent encapsulated bacterial infections commencing 30 months following the initiation of tirabrutinib (Figure S1B). No hypogammaglobulinemia nor infections were observed in the other two patients. This phenotype was not observed in this cohort in those with a shorter duration or depth of response.</p><p>From sequencing data, we derived patient-specific ddPCR assays to monitor both t(11;14)(q13;q32) translocation breakpoint and point mutations (Table S3). In serial cellular and plasma DNA samples, all cases initially showed clearance of tumor DNA from the peripheral blood either as ctDNA or genomic (g) DNA derived from circulating tumor cells (CTC) (Figure 1A–C and Figure S2). In the two relapsing patients it was possible to detect recurrent tumor DNA in peripheral blood either as plasma ctDNA or CTC genomic DNA (gDNA), 3 months, and 14 months, prior to radiological and clinical relapse. In patient 201-162, the disease remains undetectable. <i>BTK</i> C481S, T474I, or L528W mutations were not detectable using ddPCR in all three patients (data not shown).</p><p>Although our data are limited by a small sample size, the three exceptional responder cases who entered durable CR with single agent BTKi lacked a common mutational signature and genetic evidence for chronic active BCR signaling. These findings identify with Wheeler et al., 2021 where the molecular basis for therapeutic success in exceptional responders was identified in less than one quarter of 111 exceptional responders [<span>12</span>].</p><p>We show that serial monitoring of plasma ctDNA and CTC gDNA samples by ddPCR demonstrated early detection of progressive disease in the context of a BTKi treatment. Similar to prior studies, tumor-specific clonotypes can be identified in MCL enabling tracking in peripheral blood. In both relapsing patients, ctDNA was more sensitive than the cellular DNA-based assay in the detection of disease re-emergence ahead of radiological and clinical relapse. These data might have permitted early initiation of CAR-T therapy before the development of rapidly progressive, overwhelming disease; some 40% of patients with R/R MCL may fail to get to CAR-T therapy due to such rapid progression [<span>15</span>].</p><p>Abdullah N. M. Alqahtani, Sandrine Jayne, Christopher S. Trethewey, Sai S. Duraisingham, and Susann Lehmann performed research. All authors were involved in data analysis and interpretation. Harriet S. Walter, Sandrine Jayne, and Martin J. S. Dyer drafted the article that was revised and approved by all authors (article writing). Martin J. S. Dyer and Harriet S. Walter designed and supervised the study.</p><p>Martin J. S. Dyer has received research funding from Gilead Sciences. Harriet S. Walter has received research funding from Gilead Sciences. Sandrine Jayne has received research funding from Gilead Sciences. All the other authors declare no conflict of interest.</p><p>This work was supported by funds from King Faisal Medical City for Southern Regions (KFMCity) (Saudi Arabia), the Scott-Waudby Trust, the Hope Against Cancer charity, Cancer Research UK in conjunction with the UK Department of Health on an Experimental Cancer Medicine Centre grant [C10604/A25151] and by Leicester Drug Discovery and Diagnostics under the University of Leicester Institute for Precision Health [MRC—Impact Acceleration Account MR/X502777/1]. This research used the Core Biotechnology Services (NUCLEUS) and the ALICE High Performance Computing Facility at the University of Leicester. The research was carried out at the National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre (BRC).</p><p>This study was approved by the local Research Ethics Committee and the University Hospitals of Leicester Nation Health Service Trust (06/Q2501/122). All patients were consented to this.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 4","pages":"896-899"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.966","citationCount":"0","resultStr":"{\"title\":\"Monitoring of molecular responses to tirabrutinib in a cohort of exceptional responders with relapsed/refractory mantle cell lymphoma\",\"authors\":\"Abdullah N. M. Alqahtani, Sandrine Jayne, Matthew J. Ahearne, Christopher S. Trethewey, Sai S. Duraisingham, Susann Lehmann, Caroline M. Cowley, Martin J. S. Dyer, Harriet S. Walter\",\"doi\":\"10.1002/jha2.966\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>To the Editor,</p><p>Inhibitors of Bruton's tyrosine kinase (BTK) in chronic lymphocytic leukemia (CLL) result in durable responses in nearly all patients [<span>1</span>]. In contrast, in more aggressive B-cell malignancies, including diffuse large B cell lymphoma (DLBCL) and mantle cell lymphoma (MCL), responses to single agent BTK inhibitors (BTKi) occur only in subsets of patients and are mostly of brief duration. However, exceptional responses may occur [<span>2-6</span>].</p><p>In relapsed/refractory (R/R) MCL, median progression-free survival (PFS) with single-agent covalent BTKi range from 12 (ibrutinib) to 20 months (acalabrutinib ACE-LY-004 NCT02213926 study) (Table S1) [<span>7-9</span>]. Analysis of responding patients in ACE-LY-004 showed that 8/29 evaluable patients eradicated minimal residual disease (MRD) using the quantitative ClonoSEQ next-generation sequencing assay of cellular peripheral blood DNA [<span>10</span>]. However, molecular determinants of responsiveness to BTKi in MCL, and clinical significance of attaining MRD negativity in this setting remain unknown.</p><p>Like acalabrutinib, tirabrutinib is a highly selective BTKi, binding covalently to BTKC481 via a reactive acyl alkyne group. Although only 16 MCL patients were treated with single-agent tirabrutinib within the POE001 phase 1 trial (NCT01659255), extended follow-up showed an estimated median PFS of 25.8 months at 3 years [<span>11</span>]. Three patients from this cohort, described below, attained complete responses lasting over 72 months, despite adverse prognostic features at diagnosis including <i>TP53</i> mutations, blastoid morphology, and refractoriness to immunochemotherapy. In these exceptional responders [<span>12</span>], we sought to determine common features or a tumoral mutational signature that might predict exceptional responsiveness. Secondly, we determined the depth of response using digital droplet PCR (ddPCR) in both plasma and cellular DNA samples and whether serial assessment of levels of cellular and plasma circulating tumor (ct) DNA samples might presage relapse.</p><p>Clinical and laboratory details of the three cases are given in Table 1. A schema of the treatment timelines is shown in Figure 1. Full materials and methods are found in the Supporting Information. The three patients (201-139, 201-162, and 201-170) were all treated at our center and received either 480 or 600 mg of tirabrutinib once per day. All entered a clinical and radiological remission. One patient (patient 201-162) with primary immunochemotherapy-refractory disease remains in complete remission (CR) > 108 months from trial initiation. However, in 2020, they developed estrogen receptor positive grade 2 invasive ductal breast cancer, necessitating temporary discontinuation of tirabrutinib for 4 months. The breast cancer was treated radically with surgical resection, post operative radiotherapy and tamoxifen. There remains no clinical or radiological evidence of recurrence. The other two patients relapsed 91 and 72 months after initiating tirabrutinib. Due to comorbidities, no further therapy was attempted in patient 201-170 and the patient died rapidly from uncontrolled disease. Patient 201-139 received rituximab, bendamustine, cytosine arabinoside, and subsequently pirtobrutinib with the aim of proceeding to chimeric antigen receptor (CAR)-T cell therapy, but failed to respond adequately.</p><p>Whole exome sequencing showed t(11;14)(q13;q32) with breakpoints in <i>CCND1</i> and <i>IGH</i> as anticipated, but there were no other common mutations (Table S2). Two patients exhibited <i>TP53</i> mutation (pL194R and pR181H), one <i>KMT2D</i> mutation (p.S2773Lfs*72), and one patient had two <i>ATM</i> mutations. All three cases showed unmutated (> 99% homology to germline) <i>IGHV</i> gene segment usage; two cases utilized <i>IGHV4-34</i>, the other <i>IGHV3-23</i>. Unmutated <i>IGHV4-34</i> is seen in 15% of MCL and in 15% of the non-germinal center subtype of DLBCL, including the MCD subgroup, sensitive to BTKi. Unmutated IGHV4-34 recognizes autoantigens on the surface of malignant B cells, shown to result in chronic active BCR signaling in activated B-cell-like DLBCL models [<span>13</span>]. At relapse, in patient 201-139 mutations in <i>PLCG2</i> (p.M1141T, 54% VAF), previously described in relapsed CLL with ibrutinib, and in <i>NFKB2</i> (p.G373_G374insEGVLC, 36% VAF) that activates the alternative nuclear factor κappa B pathway were seen. No <i>BTK</i> mutations were present, supporting prior findings [<span>14</span>].</p><p>Interestingly, in all 3 cases, we observed a complete absence of peripheral blood CD19+ B cells with tirabrutinib, consistent with B cell aplasia. In one case (201-139) bone marrow analysis confirmed a B-cell differentiation block at the CD19+ CD38+ sIg- B-cell precursor stage (Figure S1A). In this patient, B cell aplasia resulted in hypogammaglobulinemia and recurrent encapsulated bacterial infections commencing 30 months following the initiation of tirabrutinib (Figure S1B). No hypogammaglobulinemia nor infections were observed in the other two patients. This phenotype was not observed in this cohort in those with a shorter duration or depth of response.</p><p>From sequencing data, we derived patient-specific ddPCR assays to monitor both t(11;14)(q13;q32) translocation breakpoint and point mutations (Table S3). In serial cellular and plasma DNA samples, all cases initially showed clearance of tumor DNA from the peripheral blood either as ctDNA or genomic (g) DNA derived from circulating tumor cells (CTC) (Figure 1A–C and Figure S2). In the two relapsing patients it was possible to detect recurrent tumor DNA in peripheral blood either as plasma ctDNA or CTC genomic DNA (gDNA), 3 months, and 14 months, prior to radiological and clinical relapse. In patient 201-162, the disease remains undetectable. <i>BTK</i> C481S, T474I, or L528W mutations were not detectable using ddPCR in all three patients (data not shown).</p><p>Although our data are limited by a small sample size, the three exceptional responder cases who entered durable CR with single agent BTKi lacked a common mutational signature and genetic evidence for chronic active BCR signaling. These findings identify with Wheeler et al., 2021 where the molecular basis for therapeutic success in exceptional responders was identified in less than one quarter of 111 exceptional responders [<span>12</span>].</p><p>We show that serial monitoring of plasma ctDNA and CTC gDNA samples by ddPCR demonstrated early detection of progressive disease in the context of a BTKi treatment. Similar to prior studies, tumor-specific clonotypes can be identified in MCL enabling tracking in peripheral blood. In both relapsing patients, ctDNA was more sensitive than the cellular DNA-based assay in the detection of disease re-emergence ahead of radiological and clinical relapse. These data might have permitted early initiation of CAR-T therapy before the development of rapidly progressive, overwhelming disease; some 40% of patients with R/R MCL may fail to get to CAR-T therapy due to such rapid progression [<span>15</span>].</p><p>Abdullah N. M. Alqahtani, Sandrine Jayne, Christopher S. Trethewey, Sai S. Duraisingham, and Susann Lehmann performed research. All authors were involved in data analysis and interpretation. Harriet S. Walter, Sandrine Jayne, and Martin J. S. Dyer drafted the article that was revised and approved by all authors (article writing). Martin J. S. Dyer and Harriet S. Walter designed and supervised the study.</p><p>Martin J. S. Dyer has received research funding from Gilead Sciences. Harriet S. Walter has received research funding from Gilead Sciences. Sandrine Jayne has received research funding from Gilead Sciences. All the other authors declare no conflict of interest.</p><p>This work was supported by funds from King Faisal Medical City for Southern Regions (KFMCity) (Saudi Arabia), the Scott-Waudby Trust, the Hope Against Cancer charity, Cancer Research UK in conjunction with the UK Department of Health on an Experimental Cancer Medicine Centre grant [C10604/A25151] and by Leicester Drug Discovery and Diagnostics under the University of Leicester Institute for Precision Health [MRC—Impact Acceleration Account MR/X502777/1]. This research used the Core Biotechnology Services (NUCLEUS) and the ALICE High Performance Computing Facility at the University of Leicester. The research was carried out at the National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre (BRC).</p><p>This study was approved by the local Research Ethics Committee and the University Hospitals of Leicester Nation Health Service Trust (06/Q2501/122). All patients were consented to this.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>\",\"PeriodicalId\":72883,\"journal\":{\"name\":\"EJHaem\",\"volume\":\"5 4\",\"pages\":\"896-899\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.966\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EJHaem\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jha2.966\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.966","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
致编辑:在慢性淋巴细胞白血病(CLL)中使用布鲁顿酪氨酸激酶(BTK)抑制剂,几乎所有患者都能产生持久的应答[1]。相比之下,在侵袭性更强的 B 细胞恶性肿瘤中,包括弥漫大 B 细胞淋巴瘤(DLBCL)和套细胞淋巴瘤(MCL),只有部分患者对单药 BTK 抑制剂(BTKi)产生反应,而且大多持续时间较短。在复发/难治性(R/R)MCL中,单药共价BTKi的中位无进展生存期(PFS)从12个月(伊布替尼)到20个月(阿卡布替尼 ACE-LY-004 NCT02213926 研究)不等(表S1)[7-9]。对 ACE-LY-004 中应答患者的分析表明,使用细胞外周血 DNA 的定量 ClonoSEQ 下一代测序测定,8/29 例可评估患者根除了最小残留病(MRD)[10]。与阿卡布替尼一样,替拉布替尼也是一种高选择性 BTKi,通过反应性酰基炔基与 BTKC481 共价结合。尽管在 POE001 1 期试验(NCT01659255)中只有 16 名 MCL 患者接受了单药替瑞布替尼治疗,但延长随访显示,3 年的中位 PFS 估计为 25.8 个月[11]。尽管诊断时存在 TP53 突变、blastoid 形态和免疫化疗耐受性等不良预后特征,但该队列中仍有三名患者获得了超过 72 个月的完全应答,详情如下。在这些特殊反应者中[12],我们试图确定可能预测特殊反应性的共同特征或肿瘤突变特征。其次,我们使用数字液滴 PCR(ddPCR)测定血浆和细胞 DNA 样本的反应深度,以及连续评估细胞和血浆循环肿瘤(ct)DNA 样本的水平是否可能预示复发。治疗时间表见图 1。全部材料和方法见辅助信息。这三名患者(201-139、201-162和201-170)均在本中心接受治疗,每天一次服用480或600毫克替瑞布替尼。所有患者都获得了临床和放射学缓解。一名原发性免疫化疗难治性患者(患者编号 201-162)在试验开始后 108 个月仍保持完全缓解(CR)。然而,在2020年,他们患上了雌激素受体阳性2级浸润性导管乳腺癌,不得不暂时停用替瑞布替尼4个月。患者接受了手术切除、术后放疗和他莫昔芬等根治性治疗。目前仍无临床或放射学证据显示复发。另外两名患者分别在服用替瑞布替尼 91 个月和 72 个月后复发。由于合并症,201-170 号患者没有尝试进一步治疗,但因病情未得到控制而迅速死亡。患者201-139接受了利妥昔单抗、苯达莫司汀、胞嘧啶阿糖胞苷治疗,随后又接受了皮罗布替尼治疗,目的是进行嵌合抗原受体(CAR)-T细胞治疗,但未能取得足够的疗效。全外显子组测序结果显示,t(11;14)(q13;q32)的断裂点在CCND1和IGH中,正如预期的那样,但没有其他常见的突变(表S2)。两名患者出现 TP53 突变(pL194R 和 pR181H),一名患者出现 KMT2D 突变(p.S2773Lfs*72),一名患者出现两个 ATM 突变。所有三个病例都显示使用了未突变(与种系同源性为99%)的IGHV基因片段;其中两个病例使用了IGHV4-34,另一个病例使用了IGHV3-23。未突变的IGHV4-34见于15%的MCL和15%的非生殖中心亚型DLBCL,包括对BTKi敏感的MCD亚组。未突变的IGHV4-34能识别恶性B细胞表面的自身抗原,在活化的B细胞样DLBCL模型中显示出长期活跃的BCR信号传导[13]。复发时,201-139 号患者的 PLCG2(p.M1141T,54% VAF)和激活替代核因子 κappa B 通路的 NFKB2(p.G373_G374insEGVLC,36% VAF)发生突变,前者曾在使用伊布替尼治疗的复发 CLL 中出现过。有趣的是,在所有 3 个病例中,我们都观察到使用替瑞布替尼后外周血 CD19+ B 细胞完全缺失,这与 B 细胞增生症一致。在一个病例(201-139)中,骨髓分析证实了 CD19+ CD38+ sIg- B 细胞前体阶段的 B 细胞分化阻滞(图 S1A)。在这名患者中,B 细胞增生导致了低丙种球蛋白血症,并在开始使用替罗瑞替尼 30 个月后出现了反复的包裹性细菌感染(图 S1B)。另外两名患者未观察到低丙种球蛋白血症或感染。
Monitoring of molecular responses to tirabrutinib in a cohort of exceptional responders with relapsed/refractory mantle cell lymphoma
To the Editor,
Inhibitors of Bruton's tyrosine kinase (BTK) in chronic lymphocytic leukemia (CLL) result in durable responses in nearly all patients [1]. In contrast, in more aggressive B-cell malignancies, including diffuse large B cell lymphoma (DLBCL) and mantle cell lymphoma (MCL), responses to single agent BTK inhibitors (BTKi) occur only in subsets of patients and are mostly of brief duration. However, exceptional responses may occur [2-6].
In relapsed/refractory (R/R) MCL, median progression-free survival (PFS) with single-agent covalent BTKi range from 12 (ibrutinib) to 20 months (acalabrutinib ACE-LY-004 NCT02213926 study) (Table S1) [7-9]. Analysis of responding patients in ACE-LY-004 showed that 8/29 evaluable patients eradicated minimal residual disease (MRD) using the quantitative ClonoSEQ next-generation sequencing assay of cellular peripheral blood DNA [10]. However, molecular determinants of responsiveness to BTKi in MCL, and clinical significance of attaining MRD negativity in this setting remain unknown.
Like acalabrutinib, tirabrutinib is a highly selective BTKi, binding covalently to BTKC481 via a reactive acyl alkyne group. Although only 16 MCL patients were treated with single-agent tirabrutinib within the POE001 phase 1 trial (NCT01659255), extended follow-up showed an estimated median PFS of 25.8 months at 3 years [11]. Three patients from this cohort, described below, attained complete responses lasting over 72 months, despite adverse prognostic features at diagnosis including TP53 mutations, blastoid morphology, and refractoriness to immunochemotherapy. In these exceptional responders [12], we sought to determine common features or a tumoral mutational signature that might predict exceptional responsiveness. Secondly, we determined the depth of response using digital droplet PCR (ddPCR) in both plasma and cellular DNA samples and whether serial assessment of levels of cellular and plasma circulating tumor (ct) DNA samples might presage relapse.
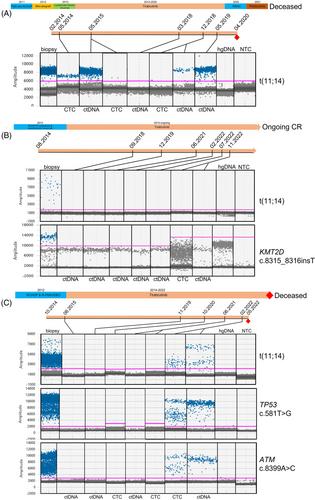
Clinical and laboratory details of the three cases are given in Table 1. A schema of the treatment timelines is shown in Figure 1. Full materials and methods are found in the Supporting Information. The three patients (201-139, 201-162, and 201-170) were all treated at our center and received either 480 or 600 mg of tirabrutinib once per day. All entered a clinical and radiological remission. One patient (patient 201-162) with primary immunochemotherapy-refractory disease remains in complete remission (CR) > 108 months from trial initiation. However, in 2020, they developed estrogen receptor positive grade 2 invasive ductal breast cancer, necessitating temporary discontinuation of tirabrutinib for 4 months. The breast cancer was treated radically with surgical resection, post operative radiotherapy and tamoxifen. There remains no clinical or radiological evidence of recurrence. The other two patients relapsed 91 and 72 months after initiating tirabrutinib. Due to comorbidities, no further therapy was attempted in patient 201-170 and the patient died rapidly from uncontrolled disease. Patient 201-139 received rituximab, bendamustine, cytosine arabinoside, and subsequently pirtobrutinib with the aim of proceeding to chimeric antigen receptor (CAR)-T cell therapy, but failed to respond adequately.
Whole exome sequencing showed t(11;14)(q13;q32) with breakpoints in CCND1 and IGH as anticipated, but there were no other common mutations (Table S2). Two patients exhibited TP53 mutation (pL194R and pR181H), one KMT2D mutation (p.S2773Lfs*72), and one patient had two ATM mutations. All three cases showed unmutated (> 99% homology to germline) IGHV gene segment usage; two cases utilized IGHV4-34, the other IGHV3-23. Unmutated IGHV4-34 is seen in 15% of MCL and in 15% of the non-germinal center subtype of DLBCL, including the MCD subgroup, sensitive to BTKi. Unmutated IGHV4-34 recognizes autoantigens on the surface of malignant B cells, shown to result in chronic active BCR signaling in activated B-cell-like DLBCL models [13]. At relapse, in patient 201-139 mutations in PLCG2 (p.M1141T, 54% VAF), previously described in relapsed CLL with ibrutinib, and in NFKB2 (p.G373_G374insEGVLC, 36% VAF) that activates the alternative nuclear factor κappa B pathway were seen. No BTK mutations were present, supporting prior findings [14].
Interestingly, in all 3 cases, we observed a complete absence of peripheral blood CD19+ B cells with tirabrutinib, consistent with B cell aplasia. In one case (201-139) bone marrow analysis confirmed a B-cell differentiation block at the CD19+ CD38+ sIg- B-cell precursor stage (Figure S1A). In this patient, B cell aplasia resulted in hypogammaglobulinemia and recurrent encapsulated bacterial infections commencing 30 months following the initiation of tirabrutinib (Figure S1B). No hypogammaglobulinemia nor infections were observed in the other two patients. This phenotype was not observed in this cohort in those with a shorter duration or depth of response.
From sequencing data, we derived patient-specific ddPCR assays to monitor both t(11;14)(q13;q32) translocation breakpoint and point mutations (Table S3). In serial cellular and plasma DNA samples, all cases initially showed clearance of tumor DNA from the peripheral blood either as ctDNA or genomic (g) DNA derived from circulating tumor cells (CTC) (Figure 1A–C and Figure S2). In the two relapsing patients it was possible to detect recurrent tumor DNA in peripheral blood either as plasma ctDNA or CTC genomic DNA (gDNA), 3 months, and 14 months, prior to radiological and clinical relapse. In patient 201-162, the disease remains undetectable. BTK C481S, T474I, or L528W mutations were not detectable using ddPCR in all three patients (data not shown).
Although our data are limited by a small sample size, the three exceptional responder cases who entered durable CR with single agent BTKi lacked a common mutational signature and genetic evidence for chronic active BCR signaling. These findings identify with Wheeler et al., 2021 where the molecular basis for therapeutic success in exceptional responders was identified in less than one quarter of 111 exceptional responders [12].
We show that serial monitoring of plasma ctDNA and CTC gDNA samples by ddPCR demonstrated early detection of progressive disease in the context of a BTKi treatment. Similar to prior studies, tumor-specific clonotypes can be identified in MCL enabling tracking in peripheral blood. In both relapsing patients, ctDNA was more sensitive than the cellular DNA-based assay in the detection of disease re-emergence ahead of radiological and clinical relapse. These data might have permitted early initiation of CAR-T therapy before the development of rapidly progressive, overwhelming disease; some 40% of patients with R/R MCL may fail to get to CAR-T therapy due to such rapid progression [15].
Abdullah N. M. Alqahtani, Sandrine Jayne, Christopher S. Trethewey, Sai S. Duraisingham, and Susann Lehmann performed research. All authors were involved in data analysis and interpretation. Harriet S. Walter, Sandrine Jayne, and Martin J. S. Dyer drafted the article that was revised and approved by all authors (article writing). Martin J. S. Dyer and Harriet S. Walter designed and supervised the study.
Martin J. S. Dyer has received research funding from Gilead Sciences. Harriet S. Walter has received research funding from Gilead Sciences. Sandrine Jayne has received research funding from Gilead Sciences. All the other authors declare no conflict of interest.
This work was supported by funds from King Faisal Medical City for Southern Regions (KFMCity) (Saudi Arabia), the Scott-Waudby Trust, the Hope Against Cancer charity, Cancer Research UK in conjunction with the UK Department of Health on an Experimental Cancer Medicine Centre grant [C10604/A25151] and by Leicester Drug Discovery and Diagnostics under the University of Leicester Institute for Precision Health [MRC—Impact Acceleration Account MR/X502777/1]. This research used the Core Biotechnology Services (NUCLEUS) and the ALICE High Performance Computing Facility at the University of Leicester. The research was carried out at the National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre (BRC).
This study was approved by the local Research Ethics Committee and the University Hospitals of Leicester Nation Health Service Trust (06/Q2501/122). All patients were consented to this.
The authors have confirmed patient consent statement is not needed for this submission.
The authors have confirmed clinical trial registration is not needed for this submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


