Christian M. Vonk, Emma L. Boertjes, Francois G. Kavelaars, Melissa Rijken, Jolinda M. L. Konijnenburg, Roxanne E. Cromwell, Bob Löwenberg, Tim Grob, Peter J. M. Valk
{"title":"在CEBPA突变的急性髓细胞性白血病中分子可测量残留病检测的预后相关性。","authors":"Christian M. Vonk, Emma L. Boertjes, Francois G. Kavelaars, Melissa Rijken, Jolinda M. L. Konijnenburg, Roxanne E. Cromwell, Bob Löwenberg, Tim Grob, Peter J. M. Valk","doi":"10.1002/hem3.141","DOIUrl":null,"url":null,"abstract":"<p>Mutations in the CCAAT/enhancer binding protein alpha (<i>CEBPA</i>) are found in 2%–15% (mean 5%) of <i>de novo</i> acute myeloid leukemia (AML) patients.<span><sup>1</sup></span> <i>CEBPA</i> encodes a transcription factor that is important for hematopoietic stem cell (HSC) self-renewal as well as myeloid differentiation of hematopoietic progenitors.<span><sup>2</sup></span> The characteristic mutations in the CEBPA protein involve frame-shift mutations in the N-terminal transactivation domains and in-frame mutations in the C-terminal basic leucine zipper (bZIP).<span><sup>2</sup></span> Recently, the in-frame <i>CEBPA</i> bZIP mutations were incorporated in the 2022 European LeukemiaNet (ELN) risk classification as a favorable risk factor,<span><sup>3</sup></span> replacing the <i>CEBPA</i> double mutations (<i>CEBPA</i><sup>dm</sup>) as favorable marker in the preceding ELN2017 guidelines.<span><sup>4</sup></span></p><p>Recent advances in molecular minimal residual disease (MRD) detection in complete remission (CR) have shown profound prognostic value of a selection of AML-specific gene mutations.<span><sup>5-7</sup></span> However, the prognostic impact of persisting <i>CEBPA</i> mutations in CR has not been thoroughly investigated in AML patients. Here, we explored the prognostic impact of mutant <i>CEBPA</i> MRD in a relatively large cohort of 84 AML patients with mutated <i>CEBPA</i> by deep next-generation sequencing (NGS).</p><p>AML patients enrolled in the Dutch-Belgian Cooperative Trial Group for Hematology-Oncology (HOVON) and Swiss Group for Clinical Cancer Research (SAKK) clinical trials HO42A, HO92, HO102, HO103, and HO132 were included. All trial participants provided written informed consent in accordance with the Declaration of Helsinki, and were treated according to their respective treatment protocol (www.hovon.nl). Patients were assessed for gene mutations on diagnostic bone marrow samples using the TruSight Myeloid Sequencing panel (Illumina) targeting 54 frequently mutated genes in AML.<span><sup>8</sup></span> Since NGS quality and depth of sequencing of the <i>CEBPA</i> gene varies when using this gene panel, <i>CEBPA</i> targeted sequencing was additionally performed on DNA of these diagnostic samples using a custom four-amplicon polymerase chain reaction (PCR) approach (amplicons A, B, C1, C2; Supporting Information: Methods).<span><sup>9</sup></span> A total of 144 <i>CEBPA</i> mutant patients out of 1913 AML cases was identified, of which 84 with available CR samples were included for mutant <i>CEBPA</i> MRD assessment. Targeted deep sequencing was performed on 100 ng of DNA obtained at CR, after two cycles of standard induction chemotherapy and pretransplant, using the four-amplicon PCR-based NGS approach.<span><sup>8, 9</sup></span></p><p>At diagnosis, 43 out of 84 cases harbored a mutation in the bZIP region (bzip), whereas 41 carried other mutations (non-bzip) (Supporting Information S1: Table 1). All <i>CEBPA</i><sup>bzip</sup> mutations were in-frame insertions. <i>CEBPA</i><sup>bzip</sup> patients were significantly younger, but no significant differences were present between <i>CEBPA</i><sup>bzip</sup> and <i>CEBPA</i><sup>non-bzip</sup> patients in terms of sex, blast, and white blood cell counts at diagnosis, consolidation therapy, or treatment protocol (Supporting Information S1: Table 2).</p><p>Mutations were subsequently classified according to the ELN2017 (single mutant: <i>CEBPA</i><sup>sm</sup> [<i>n</i> = 28] vs. double mutant: <i>CEBPA</i><sup>dm</sup> [<i>n</i> = 56]) and ELN2022 (<i>CEBPA</i><sup>bzip</sup> [<i>n</i> = 43] and <i>CEBPA</i><sup>non-bzip</sup> [<i>n</i> = 41]) risk stratifications (Supporting Information S1: Figure 1). All <i>CEBPA</i><sup>bzip</sup> patients remained part of the favorable risk group in ELN2022, whereas <i>CEBPA</i><sup>non-bzip</sup> AML patients were stratified into favorable (27%), intermediate (39%), or adverse (34%) risk groups according to the ELN2022 criteria. Compared to ELN2017, 17 out of 84 <i>CEBPA</i> mutant AML patients were re-stratified into a different risk ELN2022 category, that is, 15 <i>CEBPA</i><sup>dm</sup> AML patients (27%) did not carry a favorable in-frame bZIP mutation, whereas two <i>CEBPA</i><sup>sm</sup> AML patients did (Supporting Information S1: Figure 1).</p><p>In the complete <i>CEBPA</i> mutant AML cohort, <i>TET2</i> was most frequently comutated (24%), followed by <i>GATA2</i> (23%), <i>NPM1</i> (17%), <i>NRAS</i> (17%), and <i>DNMT3A</i> (16%) (Supporting Information S1: Figure 2). Six <i>CEBPA</i> mutant AML patients did not have any known co-mutation. <i>NPM1</i> (32%, <i>p</i> < 0.001), <i>DNMT3A</i> (27%, <i>p</i> = 0.006), <i>SRSF2</i> (20%, <i>p</i> = 0.014), <i>RUNX1</i> (17%, <i>p</i> = 0.028), <i>IDH2</i> (17%, <i>p</i> = 0.005), <i>ASXL1</i> (15%, <i>p</i> = 0.011), <i>FLT3</i>-TKD (15%, <i>p</i> = 0.011), and <i>IDH1</i> (12%, <i>p</i> = 0.024) were significantly more often mutated in <i>CEBPA</i><sup>non-bzip</sup> patients, whereas mutations in <i>GATA2</i> (40%, <i>p</i> < 0.001) and <i>WT1</i> (23%, <i>p</i> = 0.026) were more frequent among <i>CEBPA</i><sup>bzip</sup> patients (Supporting Information S1: Figure 2).</p><p>Next, we examined the differences in clinical outcome between the different <i>CEBPA</i> mutant AML subgroups. Overall survival (OS) and cumulative incidence of relapse (CIR) were compared between the subgroups using Kaplan–Meier estimates for all AML patients with mutant <i>CEBPA</i> at diagnosis (<i>n</i> = 84). OS and CIR were calculated from the date of sampling in CR to the date of an event. As expected, the presence of a <i>CEBPA</i><sup>bzip</sup> mutation at diagnosis was associated with improved OS compared to <i>CEBPA</i><sup>non-bzip</sup> mutations (<i>p</i> = 0.05).<span><sup>10, 11</sup></span> No significant difference was observed in CIR (Supporting Information S1: Figure 3).</p><p>Altogether, these characteristics demonstrate that our cohort of 84 AML cases is representative for <i>CEBPA</i>-mutated AML.<span><sup>10, 11</sup></span></p><p>The presence of mutant <i>CEBPA</i> MRD was determined using NGS deep sequencing (average read depth: 579,164<b>×</b>, range: 97,806<b>×</b>–1,566,187<b>×</b>) enabling detection of mutant <i>CEBPA</i> at a sensitivity up to 0.0004% VAF (VAF ≥ 0.0004% [indel, <i>n</i> = 58] and ≥0.03% [SNV, <i>n</i> = 3]; Supporting Information S1: Figure 4).<span><sup>9</sup></span> Persistence of <i>CEBPA</i> mutations was demonstrated in 42 out of 84 mutant <i>CEBPA</i> AML cases. Allogeneic hematopoietic stem cell transplantation (HSCT) was carried out in 23 patients (27%, Supporting Information S1: Table 2), and censoring at allogeneic HSCT was performed in all survival analyses. In AML patients with detectable <i>CEBPA</i> MRD regardless of mutation type, relapse rates were increased and OS was inferior although not statistically significant (<i>p</i> = 0.24 and <i>p</i> = 0.49 respectively; Figure 1A,B). In addition, multiparameter flow cytometry (MFC) MRD was assessed in 68 out of 84 mutant <i>CEBPA</i> AML patients. Twelve had detectable MFC-MRD (18%), and did not correlate with mutant <i>CEBPA</i> MRD status. Detection of MFC-MRD did not lead to a significantly increased CIR or inferior OS in mutant <i>CEBPA</i> AML patients (Supporting Information S1: Figure 5). Due to the low number of MFC-MRD-positive cases, no further analyses could be performed.</p><p>We next addressed the association of MRD and outcome according to <i>CEBPA</i> mutation type. <i>CEBPA</i><sup>bzip</sup> MRD was detectable in 22 out of 43 patients (51%), whereas <i>CEBPA</i><sup>non-bzip</sup> MRD was present in 20 out of 41 patients (49%). Patient characteristics did not significantly differ between different MRD status within the <i>CEBPA</i><sup>bzip</sup> and <i>CEBPA</i><sup>non-bzip</sup> subgroups (Supporting Information S1: Tables 3 and 4). Persisting <i>CEBPA</i><sup>bzip</sup> in CR did not associate with changes in OS or CIR (Figure 1C,D). In contrast, detectable MRD in <i>CEBPA</i><sup>non-bzip</sup> AML patients showed a nonsignificant trend towards increased CIR and inferior OS (<i>p</i> = 0.12 and <i>p</i> = 0.24; Figure 1E,F). Importantly, an increase in 2-year relapse risk was seen for <i>CEBPA</i><sup>non-bzip</sup> AML patients with detectable MRD (2-year CIR: 59%) compared to patients without (2-year CIR: 26%), indicating that <i>CEBPA</i><sup>non-bzip</sup> MRD is potentially a strong prognostic factor for relapse risk, independent of allogeneic HSCT. In sensitivity analysis, no significant age-related or trial-related interactions were observed. The number of cases did not allow multivariable analyses.</p><p>The persistence of co-existing mutations in <i>NPM1</i> (<i>n</i> = 13) and <i>FLT3</i> internal tandem duplication (ITD) (<i>n</i> = 10) in CR was also determined using NGS deep sequencing.<span><sup>7</sup></span> Out of 12 mutant <i>NPM1/CEBPA</i><sup>non-bzip</sup> AML patients, five had detectable mutant <i>NPM1</i> MRD, of which three also had <i>CEBPA</i><sup>non-bzip</sup> MRD. Moreover, three out of five <i>FLT3</i>-ITD/<i>CEBPA</i><sup>non-bzip</sup> AML patients had detectable <i>FLT3</i>-ITD in CR, all in combination with detectable <i>CEBPA</i><sup>non-bzip</sup> MRD. None of the four <i>FLT3</i>-ITD/<i>CEBPA</i><sup>bzip</sup> patients had detectable <i>FLT3</i>-ITD MRD, while <i>CEBPA</i><sup>bzip</sup> persisted in three of these patients. All AML patients with detectable <i>FLT3</i>-ITD MRD and three out of five with detectable mutant <i>NPM1</i> MRD experienced relapse, possibly explaining the trend in increased CIR seen in patients with <i>CEBPA</i><sup>non-bzip</sup> MRD (Figure 1E). However, larger studies are needed to demonstrate whether persistence of these secondary persisting mutations is associated with increased CIR.</p><p>In conclusion, we have studied mutant <i>CEBPA</i> MRD in a representative <i>CEBPA-</i>mutated AML cohort, that is, our data support previous findings that <i>CEBPA</i><sup>bzip</sup> mutations are present in younger AML patients, carry specific co-mutations and confer improved OS in <i>CEBPA</i>-mutated AML.<span><sup>10, 11</sup></span> Here we show in a relatively large cohort of 84 AML patients, that mutant <i>CEBPA</i> MRD is not significantly associated with increased CIR or inferior OS. Importantly, we demonstrate that mutant <i>CEBPA</i> MRD in the ELN2022 favorable subtype of AML carrying <i>CEBPA</i><sup>bzip</sup> mutations does not have impact on outcome. However, AML patients carrying persistent <i>CEBPA</i><sup>non-bzip</sup> mutations in CR have increased CIR and inferior OS. We were unable to demonstrate whether this association was independent of other risk factors. In fact, mutant <i>NPM1</i> or <i>FLT3</i>-ITD persisting in CR might be better indicators for impending relapse in <i>CEBPA</i><sup>non-bzip</sup> AML, however, similar studies in larger <i>CEBPA-</i>mutated AML cohorts are warranted.</p><p>Christian M. Vonk, Melissa Rijken, and Francois G. Kavelaars performed experiments. Christian M. Vonk, Emma L. Boertjes, Roxanne E. Cromwell, Francois G. Kavelaars, Jolinda M. L. Konijnenburg, and Tim Grob analyzed data. Christian M. Vonk, Emma L. Boertjes, and Tim Grob prepared the figures. Christian M. Vonk and Emma L. Boertjes drafted the manuscript, and all authors approved the final version of the manuscript.</p><p>The authors declare no conflict of interest.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 8","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11326717/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic relevance of molecular measurable residual disease detection in AML with mutated CEBPA\",\"authors\":\"Christian M. Vonk, Emma L. Boertjes, Francois G. Kavelaars, Melissa Rijken, Jolinda M. L. Konijnenburg, Roxanne E. Cromwell, Bob Löwenberg, Tim Grob, Peter J. M. Valk\",\"doi\":\"10.1002/hem3.141\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Mutations in the CCAAT/enhancer binding protein alpha (<i>CEBPA</i>) are found in 2%–15% (mean 5%) of <i>de novo</i> acute myeloid leukemia (AML) patients.<span><sup>1</sup></span> <i>CEBPA</i> encodes a transcription factor that is important for hematopoietic stem cell (HSC) self-renewal as well as myeloid differentiation of hematopoietic progenitors.<span><sup>2</sup></span> The characteristic mutations in the CEBPA protein involve frame-shift mutations in the N-terminal transactivation domains and in-frame mutations in the C-terminal basic leucine zipper (bZIP).<span><sup>2</sup></span> Recently, the in-frame <i>CEBPA</i> bZIP mutations were incorporated in the 2022 European LeukemiaNet (ELN) risk classification as a favorable risk factor,<span><sup>3</sup></span> replacing the <i>CEBPA</i> double mutations (<i>CEBPA</i><sup>dm</sup>) as favorable marker in the preceding ELN2017 guidelines.<span><sup>4</sup></span></p><p>Recent advances in molecular minimal residual disease (MRD) detection in complete remission (CR) have shown profound prognostic value of a selection of AML-specific gene mutations.<span><sup>5-7</sup></span> However, the prognostic impact of persisting <i>CEBPA</i> mutations in CR has not been thoroughly investigated in AML patients. Here, we explored the prognostic impact of mutant <i>CEBPA</i> MRD in a relatively large cohort of 84 AML patients with mutated <i>CEBPA</i> by deep next-generation sequencing (NGS).</p><p>AML patients enrolled in the Dutch-Belgian Cooperative Trial Group for Hematology-Oncology (HOVON) and Swiss Group for Clinical Cancer Research (SAKK) clinical trials HO42A, HO92, HO102, HO103, and HO132 were included. All trial participants provided written informed consent in accordance with the Declaration of Helsinki, and were treated according to their respective treatment protocol (www.hovon.nl). Patients were assessed for gene mutations on diagnostic bone marrow samples using the TruSight Myeloid Sequencing panel (Illumina) targeting 54 frequently mutated genes in AML.<span><sup>8</sup></span> Since NGS quality and depth of sequencing of the <i>CEBPA</i> gene varies when using this gene panel, <i>CEBPA</i> targeted sequencing was additionally performed on DNA of these diagnostic samples using a custom four-amplicon polymerase chain reaction (PCR) approach (amplicons A, B, C1, C2; Supporting Information: Methods).<span><sup>9</sup></span> A total of 144 <i>CEBPA</i> mutant patients out of 1913 AML cases was identified, of which 84 with available CR samples were included for mutant <i>CEBPA</i> MRD assessment. Targeted deep sequencing was performed on 100 ng of DNA obtained at CR, after two cycles of standard induction chemotherapy and pretransplant, using the four-amplicon PCR-based NGS approach.<span><sup>8, 9</sup></span></p><p>At diagnosis, 43 out of 84 cases harbored a mutation in the bZIP region (bzip), whereas 41 carried other mutations (non-bzip) (Supporting Information S1: Table 1). All <i>CEBPA</i><sup>bzip</sup> mutations were in-frame insertions. <i>CEBPA</i><sup>bzip</sup> patients were significantly younger, but no significant differences were present between <i>CEBPA</i><sup>bzip</sup> and <i>CEBPA</i><sup>non-bzip</sup> patients in terms of sex, blast, and white blood cell counts at diagnosis, consolidation therapy, or treatment protocol (Supporting Information S1: Table 2).</p><p>Mutations were subsequently classified according to the ELN2017 (single mutant: <i>CEBPA</i><sup>sm</sup> [<i>n</i> = 28] vs. double mutant: <i>CEBPA</i><sup>dm</sup> [<i>n</i> = 56]) and ELN2022 (<i>CEBPA</i><sup>bzip</sup> [<i>n</i> = 43] and <i>CEBPA</i><sup>non-bzip</sup> [<i>n</i> = 41]) risk stratifications (Supporting Information S1: Figure 1). All <i>CEBPA</i><sup>bzip</sup> patients remained part of the favorable risk group in ELN2022, whereas <i>CEBPA</i><sup>non-bzip</sup> AML patients were stratified into favorable (27%), intermediate (39%), or adverse (34%) risk groups according to the ELN2022 criteria. Compared to ELN2017, 17 out of 84 <i>CEBPA</i> mutant AML patients were re-stratified into a different risk ELN2022 category, that is, 15 <i>CEBPA</i><sup>dm</sup> AML patients (27%) did not carry a favorable in-frame bZIP mutation, whereas two <i>CEBPA</i><sup>sm</sup> AML patients did (Supporting Information S1: Figure 1).</p><p>In the complete <i>CEBPA</i> mutant AML cohort, <i>TET2</i> was most frequently comutated (24%), followed by <i>GATA2</i> (23%), <i>NPM1</i> (17%), <i>NRAS</i> (17%), and <i>DNMT3A</i> (16%) (Supporting Information S1: Figure 2). Six <i>CEBPA</i> mutant AML patients did not have any known co-mutation. <i>NPM1</i> (32%, <i>p</i> < 0.001), <i>DNMT3A</i> (27%, <i>p</i> = 0.006), <i>SRSF2</i> (20%, <i>p</i> = 0.014), <i>RUNX1</i> (17%, <i>p</i> = 0.028), <i>IDH2</i> (17%, <i>p</i> = 0.005), <i>ASXL1</i> (15%, <i>p</i> = 0.011), <i>FLT3</i>-TKD (15%, <i>p</i> = 0.011), and <i>IDH1</i> (12%, <i>p</i> = 0.024) were significantly more often mutated in <i>CEBPA</i><sup>non-bzip</sup> patients, whereas mutations in <i>GATA2</i> (40%, <i>p</i> < 0.001) and <i>WT1</i> (23%, <i>p</i> = 0.026) were more frequent among <i>CEBPA</i><sup>bzip</sup> patients (Supporting Information S1: Figure 2).</p><p>Next, we examined the differences in clinical outcome between the different <i>CEBPA</i> mutant AML subgroups. Overall survival (OS) and cumulative incidence of relapse (CIR) were compared between the subgroups using Kaplan–Meier estimates for all AML patients with mutant <i>CEBPA</i> at diagnosis (<i>n</i> = 84). OS and CIR were calculated from the date of sampling in CR to the date of an event. As expected, the presence of a <i>CEBPA</i><sup>bzip</sup> mutation at diagnosis was associated with improved OS compared to <i>CEBPA</i><sup>non-bzip</sup> mutations (<i>p</i> = 0.05).<span><sup>10, 11</sup></span> No significant difference was observed in CIR (Supporting Information S1: Figure 3).</p><p>Altogether, these characteristics demonstrate that our cohort of 84 AML cases is representative for <i>CEBPA</i>-mutated AML.<span><sup>10, 11</sup></span></p><p>The presence of mutant <i>CEBPA</i> MRD was determined using NGS deep sequencing (average read depth: 579,164<b>×</b>, range: 97,806<b>×</b>–1,566,187<b>×</b>) enabling detection of mutant <i>CEBPA</i> at a sensitivity up to 0.0004% VAF (VAF ≥ 0.0004% [indel, <i>n</i> = 58] and ≥0.03% [SNV, <i>n</i> = 3]; Supporting Information S1: Figure 4).<span><sup>9</sup></span> Persistence of <i>CEBPA</i> mutations was demonstrated in 42 out of 84 mutant <i>CEBPA</i> AML cases. Allogeneic hematopoietic stem cell transplantation (HSCT) was carried out in 23 patients (27%, Supporting Information S1: Table 2), and censoring at allogeneic HSCT was performed in all survival analyses. In AML patients with detectable <i>CEBPA</i> MRD regardless of mutation type, relapse rates were increased and OS was inferior although not statistically significant (<i>p</i> = 0.24 and <i>p</i> = 0.49 respectively; Figure 1A,B). In addition, multiparameter flow cytometry (MFC) MRD was assessed in 68 out of 84 mutant <i>CEBPA</i> AML patients. Twelve had detectable MFC-MRD (18%), and did not correlate with mutant <i>CEBPA</i> MRD status. Detection of MFC-MRD did not lead to a significantly increased CIR or inferior OS in mutant <i>CEBPA</i> AML patients (Supporting Information S1: Figure 5). Due to the low number of MFC-MRD-positive cases, no further analyses could be performed.</p><p>We next addressed the association of MRD and outcome according to <i>CEBPA</i> mutation type. <i>CEBPA</i><sup>bzip</sup> MRD was detectable in 22 out of 43 patients (51%), whereas <i>CEBPA</i><sup>non-bzip</sup> MRD was present in 20 out of 41 patients (49%). Patient characteristics did not significantly differ between different MRD status within the <i>CEBPA</i><sup>bzip</sup> and <i>CEBPA</i><sup>non-bzip</sup> subgroups (Supporting Information S1: Tables 3 and 4). Persisting <i>CEBPA</i><sup>bzip</sup> in CR did not associate with changes in OS or CIR (Figure 1C,D). In contrast, detectable MRD in <i>CEBPA</i><sup>non-bzip</sup> AML patients showed a nonsignificant trend towards increased CIR and inferior OS (<i>p</i> = 0.12 and <i>p</i> = 0.24; Figure 1E,F). Importantly, an increase in 2-year relapse risk was seen for <i>CEBPA</i><sup>non-bzip</sup> AML patients with detectable MRD (2-year CIR: 59%) compared to patients without (2-year CIR: 26%), indicating that <i>CEBPA</i><sup>non-bzip</sup> MRD is potentially a strong prognostic factor for relapse risk, independent of allogeneic HSCT. In sensitivity analysis, no significant age-related or trial-related interactions were observed. The number of cases did not allow multivariable analyses.</p><p>The persistence of co-existing mutations in <i>NPM1</i> (<i>n</i> = 13) and <i>FLT3</i> internal tandem duplication (ITD) (<i>n</i> = 10) in CR was also determined using NGS deep sequencing.<span><sup>7</sup></span> Out of 12 mutant <i>NPM1/CEBPA</i><sup>non-bzip</sup> AML patients, five had detectable mutant <i>NPM1</i> MRD, of which three also had <i>CEBPA</i><sup>non-bzip</sup> MRD. Moreover, three out of five <i>FLT3</i>-ITD/<i>CEBPA</i><sup>non-bzip</sup> AML patients had detectable <i>FLT3</i>-ITD in CR, all in combination with detectable <i>CEBPA</i><sup>non-bzip</sup> MRD. None of the four <i>FLT3</i>-ITD/<i>CEBPA</i><sup>bzip</sup> patients had detectable <i>FLT3</i>-ITD MRD, while <i>CEBPA</i><sup>bzip</sup> persisted in three of these patients. All AML patients with detectable <i>FLT3</i>-ITD MRD and three out of five with detectable mutant <i>NPM1</i> MRD experienced relapse, possibly explaining the trend in increased CIR seen in patients with <i>CEBPA</i><sup>non-bzip</sup> MRD (Figure 1E). However, larger studies are needed to demonstrate whether persistence of these secondary persisting mutations is associated with increased CIR.</p><p>In conclusion, we have studied mutant <i>CEBPA</i> MRD in a representative <i>CEBPA-</i>mutated AML cohort, that is, our data support previous findings that <i>CEBPA</i><sup>bzip</sup> mutations are present in younger AML patients, carry specific co-mutations and confer improved OS in <i>CEBPA</i>-mutated AML.<span><sup>10, 11</sup></span> Here we show in a relatively large cohort of 84 AML patients, that mutant <i>CEBPA</i> MRD is not significantly associated with increased CIR or inferior OS. Importantly, we demonstrate that mutant <i>CEBPA</i> MRD in the ELN2022 favorable subtype of AML carrying <i>CEBPA</i><sup>bzip</sup> mutations does not have impact on outcome. However, AML patients carrying persistent <i>CEBPA</i><sup>non-bzip</sup> mutations in CR have increased CIR and inferior OS. We were unable to demonstrate whether this association was independent of other risk factors. In fact, mutant <i>NPM1</i> or <i>FLT3</i>-ITD persisting in CR might be better indicators for impending relapse in <i>CEBPA</i><sup>non-bzip</sup> AML, however, similar studies in larger <i>CEBPA-</i>mutated AML cohorts are warranted.</p><p>Christian M. Vonk, Melissa Rijken, and Francois G. Kavelaars performed experiments. Christian M. Vonk, Emma L. Boertjes, Roxanne E. Cromwell, Francois G. Kavelaars, Jolinda M. L. Konijnenburg, and Tim Grob analyzed data. Christian M. Vonk, Emma L. Boertjes, and Tim Grob prepared the figures. Christian M. Vonk and Emma L. Boertjes drafted the manuscript, and all authors approved the final version of the manuscript.</p><p>The authors declare no conflict of interest.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 8\",\"pages\":\"\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2024-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11326717/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.141\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.141","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Prognostic relevance of molecular measurable residual disease detection in AML with mutated CEBPA
Mutations in the CCAAT/enhancer binding protein alpha (CEBPA) are found in 2%–15% (mean 5%) of de novo acute myeloid leukemia (AML) patients.1CEBPA encodes a transcription factor that is important for hematopoietic stem cell (HSC) self-renewal as well as myeloid differentiation of hematopoietic progenitors.2 The characteristic mutations in the CEBPA protein involve frame-shift mutations in the N-terminal transactivation domains and in-frame mutations in the C-terminal basic leucine zipper (bZIP).2 Recently, the in-frame CEBPA bZIP mutations were incorporated in the 2022 European LeukemiaNet (ELN) risk classification as a favorable risk factor,3 replacing the CEBPA double mutations (CEBPAdm) as favorable marker in the preceding ELN2017 guidelines.4
Recent advances in molecular minimal residual disease (MRD) detection in complete remission (CR) have shown profound prognostic value of a selection of AML-specific gene mutations.5-7 However, the prognostic impact of persisting CEBPA mutations in CR has not been thoroughly investigated in AML patients. Here, we explored the prognostic impact of mutant CEBPA MRD in a relatively large cohort of 84 AML patients with mutated CEBPA by deep next-generation sequencing (NGS).
AML patients enrolled in the Dutch-Belgian Cooperative Trial Group for Hematology-Oncology (HOVON) and Swiss Group for Clinical Cancer Research (SAKK) clinical trials HO42A, HO92, HO102, HO103, and HO132 were included. All trial participants provided written informed consent in accordance with the Declaration of Helsinki, and were treated according to their respective treatment protocol (www.hovon.nl). Patients were assessed for gene mutations on diagnostic bone marrow samples using the TruSight Myeloid Sequencing panel (Illumina) targeting 54 frequently mutated genes in AML.8 Since NGS quality and depth of sequencing of the CEBPA gene varies when using this gene panel, CEBPA targeted sequencing was additionally performed on DNA of these diagnostic samples using a custom four-amplicon polymerase chain reaction (PCR) approach (amplicons A, B, C1, C2; Supporting Information: Methods).9 A total of 144 CEBPA mutant patients out of 1913 AML cases was identified, of which 84 with available CR samples were included for mutant CEBPA MRD assessment. Targeted deep sequencing was performed on 100 ng of DNA obtained at CR, after two cycles of standard induction chemotherapy and pretransplant, using the four-amplicon PCR-based NGS approach.8, 9
At diagnosis, 43 out of 84 cases harbored a mutation in the bZIP region (bzip), whereas 41 carried other mutations (non-bzip) (Supporting Information S1: Table 1). All CEBPAbzip mutations were in-frame insertions. CEBPAbzip patients were significantly younger, but no significant differences were present between CEBPAbzip and CEBPAnon-bzip patients in terms of sex, blast, and white blood cell counts at diagnosis, consolidation therapy, or treatment protocol (Supporting Information S1: Table 2).
Mutations were subsequently classified according to the ELN2017 (single mutant: CEBPAsm [n = 28] vs. double mutant: CEBPAdm [n = 56]) and ELN2022 (CEBPAbzip [n = 43] and CEBPAnon-bzip [n = 41]) risk stratifications (Supporting Information S1: Figure 1). All CEBPAbzip patients remained part of the favorable risk group in ELN2022, whereas CEBPAnon-bzip AML patients were stratified into favorable (27%), intermediate (39%), or adverse (34%) risk groups according to the ELN2022 criteria. Compared to ELN2017, 17 out of 84 CEBPA mutant AML patients were re-stratified into a different risk ELN2022 category, that is, 15 CEBPAdm AML patients (27%) did not carry a favorable in-frame bZIP mutation, whereas two CEBPAsm AML patients did (Supporting Information S1: Figure 1).
In the complete CEBPA mutant AML cohort, TET2 was most frequently comutated (24%), followed by GATA2 (23%), NPM1 (17%), NRAS (17%), and DNMT3A (16%) (Supporting Information S1: Figure 2). Six CEBPA mutant AML patients did not have any known co-mutation. NPM1 (32%, p < 0.001), DNMT3A (27%, p = 0.006), SRSF2 (20%, p = 0.014), RUNX1 (17%, p = 0.028), IDH2 (17%, p = 0.005), ASXL1 (15%, p = 0.011), FLT3-TKD (15%, p = 0.011), and IDH1 (12%, p = 0.024) were significantly more often mutated in CEBPAnon-bzip patients, whereas mutations in GATA2 (40%, p < 0.001) and WT1 (23%, p = 0.026) were more frequent among CEBPAbzip patients (Supporting Information S1: Figure 2).
Next, we examined the differences in clinical outcome between the different CEBPA mutant AML subgroups. Overall survival (OS) and cumulative incidence of relapse (CIR) were compared between the subgroups using Kaplan–Meier estimates for all AML patients with mutant CEBPA at diagnosis (n = 84). OS and CIR were calculated from the date of sampling in CR to the date of an event. As expected, the presence of a CEBPAbzip mutation at diagnosis was associated with improved OS compared to CEBPAnon-bzip mutations (p = 0.05).10, 11 No significant difference was observed in CIR (Supporting Information S1: Figure 3).
Altogether, these characteristics demonstrate that our cohort of 84 AML cases is representative for CEBPA-mutated AML.10, 11
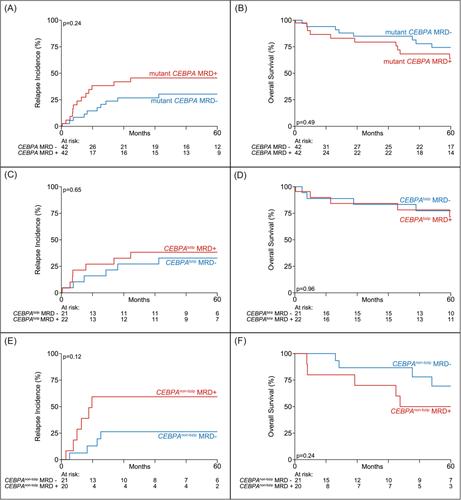
The presence of mutant CEBPA MRD was determined using NGS deep sequencing (average read depth: 579,164×, range: 97,806×–1,566,187×) enabling detection of mutant CEBPA at a sensitivity up to 0.0004% VAF (VAF ≥ 0.0004% [indel, n = 58] and ≥0.03% [SNV, n = 3]; Supporting Information S1: Figure 4).9 Persistence of CEBPA mutations was demonstrated in 42 out of 84 mutant CEBPA AML cases. Allogeneic hematopoietic stem cell transplantation (HSCT) was carried out in 23 patients (27%, Supporting Information S1: Table 2), and censoring at allogeneic HSCT was performed in all survival analyses. In AML patients with detectable CEBPA MRD regardless of mutation type, relapse rates were increased and OS was inferior although not statistically significant (p = 0.24 and p = 0.49 respectively; Figure 1A,B). In addition, multiparameter flow cytometry (MFC) MRD was assessed in 68 out of 84 mutant CEBPA AML patients. Twelve had detectable MFC-MRD (18%), and did not correlate with mutant CEBPA MRD status. Detection of MFC-MRD did not lead to a significantly increased CIR or inferior OS in mutant CEBPA AML patients (Supporting Information S1: Figure 5). Due to the low number of MFC-MRD-positive cases, no further analyses could be performed.
We next addressed the association of MRD and outcome according to CEBPA mutation type. CEBPAbzip MRD was detectable in 22 out of 43 patients (51%), whereas CEBPAnon-bzip MRD was present in 20 out of 41 patients (49%). Patient characteristics did not significantly differ between different MRD status within the CEBPAbzip and CEBPAnon-bzip subgroups (Supporting Information S1: Tables 3 and 4). Persisting CEBPAbzip in CR did not associate with changes in OS or CIR (Figure 1C,D). In contrast, detectable MRD in CEBPAnon-bzip AML patients showed a nonsignificant trend towards increased CIR and inferior OS (p = 0.12 and p = 0.24; Figure 1E,F). Importantly, an increase in 2-year relapse risk was seen for CEBPAnon-bzip AML patients with detectable MRD (2-year CIR: 59%) compared to patients without (2-year CIR: 26%), indicating that CEBPAnon-bzip MRD is potentially a strong prognostic factor for relapse risk, independent of allogeneic HSCT. In sensitivity analysis, no significant age-related or trial-related interactions were observed. The number of cases did not allow multivariable analyses.
The persistence of co-existing mutations in NPM1 (n = 13) and FLT3 internal tandem duplication (ITD) (n = 10) in CR was also determined using NGS deep sequencing.7 Out of 12 mutant NPM1/CEBPAnon-bzip AML patients, five had detectable mutant NPM1 MRD, of which three also had CEBPAnon-bzip MRD. Moreover, three out of five FLT3-ITD/CEBPAnon-bzip AML patients had detectable FLT3-ITD in CR, all in combination with detectable CEBPAnon-bzip MRD. None of the four FLT3-ITD/CEBPAbzip patients had detectable FLT3-ITD MRD, while CEBPAbzip persisted in three of these patients. All AML patients with detectable FLT3-ITD MRD and three out of five with detectable mutant NPM1 MRD experienced relapse, possibly explaining the trend in increased CIR seen in patients with CEBPAnon-bzip MRD (Figure 1E). However, larger studies are needed to demonstrate whether persistence of these secondary persisting mutations is associated with increased CIR.
In conclusion, we have studied mutant CEBPA MRD in a representative CEBPA-mutated AML cohort, that is, our data support previous findings that CEBPAbzip mutations are present in younger AML patients, carry specific co-mutations and confer improved OS in CEBPA-mutated AML.10, 11 Here we show in a relatively large cohort of 84 AML patients, that mutant CEBPA MRD is not significantly associated with increased CIR or inferior OS. Importantly, we demonstrate that mutant CEBPA MRD in the ELN2022 favorable subtype of AML carrying CEBPAbzip mutations does not have impact on outcome. However, AML patients carrying persistent CEBPAnon-bzip mutations in CR have increased CIR and inferior OS. We were unable to demonstrate whether this association was independent of other risk factors. In fact, mutant NPM1 or FLT3-ITD persisting in CR might be better indicators for impending relapse in CEBPAnon-bzip AML, however, similar studies in larger CEBPA-mutated AML cohorts are warranted.
Christian M. Vonk, Melissa Rijken, and Francois G. Kavelaars performed experiments. Christian M. Vonk, Emma L. Boertjes, Roxanne E. Cromwell, Francois G. Kavelaars, Jolinda M. L. Konijnenburg, and Tim Grob analyzed data. Christian M. Vonk, Emma L. Boertjes, and Tim Grob prepared the figures. Christian M. Vonk and Emma L. Boertjes drafted the manuscript, and all authors approved the final version of the manuscript.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


