Carine E Hamo, Colette DeJong, Nick Hartshorne-Evans, Lars H Lund, Sanjiv J Shah, Scott Solomon, Carolyn S P Lam
{"title":"射血分数保留型心力衰竭","authors":"Carine E Hamo, Colette DeJong, Nick Hartshorne-Evans, Lars H Lund, Sanjiv J Shah, Scott Solomon, Carolyn S P Lam","doi":"10.1038/s41572-024-00540-y","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure with preserved ejection fraction (HFpEF) accounts for nearly half of all heart failure cases and has a prevalence that is expected to rise with the growing ageing population. HFpEF is associated with significant morbidity and mortality. Specific HFpEF risk factors include age, diabetes, hypertension, obesity and atrial fibrillation. Haemodynamic contributions to HFpEF include changes in left ventricular structure, diastolic and systolic dysfunction, left atrial myopathy, pulmonary hypertension, right ventricular dysfunction, chronotropic incompetence, and vascular dysfunction. Inflammation, fibrosis, impaired nitric oxide signalling, sarcomere dysfunction, and mitochondrial and metabolic defects contribute to the cellular and molecular changes observed in HFpEF. HFpEF impacts multiple organ systems beyond the heart, including the skeletal muscle, peripheral vasculature, lungs, kidneys and brain. The diagnosis of HFpEF can be made in individuals with signs and symptoms of heart failure with abnormality in natriuretic peptide levels or evidence of cardiopulmonary congestion, facilitated by the use of HFpEF risk scores and additional imaging and testing with the exclusion of HFpEF mimics. Management includes initiation of guideline-directed medical therapy and management of comorbidities. Given the significant impact of HFpEF on quality of life, future research efforts should include a particular focus on how patients can live better with this disease.</p>","PeriodicalId":18910,"journal":{"name":"Nature Reviews Disease Primers","volume":"10 1","pages":"55"},"PeriodicalIF":76.9000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Heart failure with preserved ejection fraction.\",\"authors\":\"Carine E Hamo, Colette DeJong, Nick Hartshorne-Evans, Lars H Lund, Sanjiv J Shah, Scott Solomon, Carolyn S P Lam\",\"doi\":\"10.1038/s41572-024-00540-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Heart failure with preserved ejection fraction (HFpEF) accounts for nearly half of all heart failure cases and has a prevalence that is expected to rise with the growing ageing population. HFpEF is associated with significant morbidity and mortality. Specific HFpEF risk factors include age, diabetes, hypertension, obesity and atrial fibrillation. Haemodynamic contributions to HFpEF include changes in left ventricular structure, diastolic and systolic dysfunction, left atrial myopathy, pulmonary hypertension, right ventricular dysfunction, chronotropic incompetence, and vascular dysfunction. Inflammation, fibrosis, impaired nitric oxide signalling, sarcomere dysfunction, and mitochondrial and metabolic defects contribute to the cellular and molecular changes observed in HFpEF. HFpEF impacts multiple organ systems beyond the heart, including the skeletal muscle, peripheral vasculature, lungs, kidneys and brain. The diagnosis of HFpEF can be made in individuals with signs and symptoms of heart failure with abnormality in natriuretic peptide levels or evidence of cardiopulmonary congestion, facilitated by the use of HFpEF risk scores and additional imaging and testing with the exclusion of HFpEF mimics. Management includes initiation of guideline-directed medical therapy and management of comorbidities. Given the significant impact of HFpEF on quality of life, future research efforts should include a particular focus on how patients can live better with this disease.</p>\",\"PeriodicalId\":18910,\"journal\":{\"name\":\"Nature Reviews Disease Primers\",\"volume\":\"10 1\",\"pages\":\"55\"},\"PeriodicalIF\":76.9000,\"publicationDate\":\"2024-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Reviews Disease Primers\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41572-024-00540-y\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Reviews Disease Primers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41572-024-00540-y","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
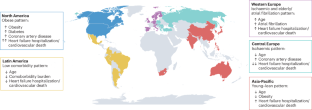
Heart failure with preserved ejection fraction (HFpEF) accounts for nearly half of all heart failure cases and has a prevalence that is expected to rise with the growing ageing population. HFpEF is associated with significant morbidity and mortality. Specific HFpEF risk factors include age, diabetes, hypertension, obesity and atrial fibrillation. Haemodynamic contributions to HFpEF include changes in left ventricular structure, diastolic and systolic dysfunction, left atrial myopathy, pulmonary hypertension, right ventricular dysfunction, chronotropic incompetence, and vascular dysfunction. Inflammation, fibrosis, impaired nitric oxide signalling, sarcomere dysfunction, and mitochondrial and metabolic defects contribute to the cellular and molecular changes observed in HFpEF. HFpEF impacts multiple organ systems beyond the heart, including the skeletal muscle, peripheral vasculature, lungs, kidneys and brain. The diagnosis of HFpEF can be made in individuals with signs and symptoms of heart failure with abnormality in natriuretic peptide levels or evidence of cardiopulmonary congestion, facilitated by the use of HFpEF risk scores and additional imaging and testing with the exclusion of HFpEF mimics. Management includes initiation of guideline-directed medical therapy and management of comorbidities. Given the significant impact of HFpEF on quality of life, future research efforts should include a particular focus on how patients can live better with this disease.
期刊介绍:
Nature Reviews Disease Primers, a part of the Nature Reviews journal portfolio, features sections on epidemiology, mechanisms, diagnosis, management, and patient quality of life. The editorial team commissions top researchers — comprising basic scientists and clinical researchers — to write the Primers, which are designed for use by early career researchers, medical students and principal investigators. Each Primer concludes with an Outlook section, highlighting future research directions. Covered medical specialties include Cardiology, Dermatology, Ear, Nose and Throat, Emergency Medicine, Endocrinology, Gastroenterology, Genetic Conditions, Gynaecology and Obstetrics, Hepatology, Haematology, Infectious Diseases, Maxillofacial and Oral Medicine, Nephrology, Neurology, Nutrition, Oncology, Ophthalmology, Orthopaedics, Psychiatry, Respiratory Medicine, Rheumatology, Sleep Medicine, and Urology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


