Manman Liu, Chao Liang, Meijing Ying, Fulvia Ortolani, Biling Wu, Jie Liu, Zhen Yang, Wanxia Xiong, Ming Ding
{"title":"术前自体富血小板血浆置换术对心脏瓣膜手术患者术后出血的影响。","authors":"Manman Liu, Chao Liang, Meijing Ying, Fulvia Ortolani, Biling Wu, Jie Liu, Zhen Yang, Wanxia Xiong, Ming Ding","doi":"10.21037/jtd-24-794","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular surgeries often require deep hypothermic circulatory arrest and cardiopulmonary bypass (CPB), which can disrupt blood clotting and lead to excessive bleeding. Traditional treatments involve transfusing blood and blood products, which can have adverse effects and place significant strain on the global blood supply. Research suggests that autologous platelet-rich plasmapheresis (aPRP) may reduce the need for transfusions by preserving blood components. However, the impact of aPRP on postoperative blood loss and clinical outcomes in cardiovascular surgery remains controversial. This study aimed to examine the effects of aPRP on postoperative blood loss and recovery in patients undergoing heart valve surgery.</p><p><strong>Methods: </strong>A total of 183 patients were divided into either aPRP or control groups. The aPRP group received aPRP before CPB, whereas the control group did not. The primary endpoint was postoperative bleeding between the groups. The secondary endpoints were postoperative bleeding risk factors and clinical outcome assessment. Logistic regression analysis with covariate adjustment was used to calculate these risk factors.</p><p><strong>Results: </strong>A total of 76 patients (41.5%) in the aPRP group and 107 patients (58.5%) in the control group were included in the analysis. No significant difference was found in the occurrence of postoperative bleeding [odds ratio (OR) =0.53, 95% confidence interval (CI): 0.28-1.00, P=0.05], and the aPRP group had fewer complications than the controls (OR =0.28, 95% CI: 0.10-0.68, P=0.009). However, after adjusting for the New York Heart Association (NYHA) classification, diabetes, arrhythmology, mean activated clotting time (ACT<sub>mean</sub>), CPB, bleeding, thoracotomy, and body mass index (BMI), there was a significant difference in postoperative bleeding (adjusted OR =0.47, 95% CI: 0.22-0.98, P=0.04) and complications (adjusted OR =0.23, 95% CI: 0.07-0.64, P=0.008) between the two groups.</p><p><strong>Conclusions: </strong>Preoperative aPRP can improve postoperative outcomes and reduce complications in patients undergoing heart valve surgery.</p>","PeriodicalId":17542,"journal":{"name":"Journal of thoracic disease","volume":"16 7","pages":"4584-4596"},"PeriodicalIF":1.9000,"publicationDate":"2024-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11320239/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of preoperative autologous platelet-rich plasmapheresis on postoperative bleeding in patients undergoing heart valve surgery.\",\"authors\":\"Manman Liu, Chao Liang, Meijing Ying, Fulvia Ortolani, Biling Wu, Jie Liu, Zhen Yang, Wanxia Xiong, Ming Ding\",\"doi\":\"10.21037/jtd-24-794\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiovascular surgeries often require deep hypothermic circulatory arrest and cardiopulmonary bypass (CPB), which can disrupt blood clotting and lead to excessive bleeding. Traditional treatments involve transfusing blood and blood products, which can have adverse effects and place significant strain on the global blood supply. Research suggests that autologous platelet-rich plasmapheresis (aPRP) may reduce the need for transfusions by preserving blood components. However, the impact of aPRP on postoperative blood loss and clinical outcomes in cardiovascular surgery remains controversial. This study aimed to examine the effects of aPRP on postoperative blood loss and recovery in patients undergoing heart valve surgery.</p><p><strong>Methods: </strong>A total of 183 patients were divided into either aPRP or control groups. The aPRP group received aPRP before CPB, whereas the control group did not. The primary endpoint was postoperative bleeding between the groups. The secondary endpoints were postoperative bleeding risk factors and clinical outcome assessment. Logistic regression analysis with covariate adjustment was used to calculate these risk factors.</p><p><strong>Results: </strong>A total of 76 patients (41.5%) in the aPRP group and 107 patients (58.5%) in the control group were included in the analysis. No significant difference was found in the occurrence of postoperative bleeding [odds ratio (OR) =0.53, 95% confidence interval (CI): 0.28-1.00, P=0.05], and the aPRP group had fewer complications than the controls (OR =0.28, 95% CI: 0.10-0.68, P=0.009). However, after adjusting for the New York Heart Association (NYHA) classification, diabetes, arrhythmology, mean activated clotting time (ACT<sub>mean</sub>), CPB, bleeding, thoracotomy, and body mass index (BMI), there was a significant difference in postoperative bleeding (adjusted OR =0.47, 95% CI: 0.22-0.98, P=0.04) and complications (adjusted OR =0.23, 95% CI: 0.07-0.64, P=0.008) between the two groups.</p><p><strong>Conclusions: </strong>Preoperative aPRP can improve postoperative outcomes and reduce complications in patients undergoing heart valve surgery.</p>\",\"PeriodicalId\":17542,\"journal\":{\"name\":\"Journal of thoracic disease\",\"volume\":\"16 7\",\"pages\":\"4584-4596\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11320239/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of thoracic disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/jtd-24-794\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of thoracic disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/jtd-24-794","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/22 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Effect of preoperative autologous platelet-rich plasmapheresis on postoperative bleeding in patients undergoing heart valve surgery.
Background: Cardiovascular surgeries often require deep hypothermic circulatory arrest and cardiopulmonary bypass (CPB), which can disrupt blood clotting and lead to excessive bleeding. Traditional treatments involve transfusing blood and blood products, which can have adverse effects and place significant strain on the global blood supply. Research suggests that autologous platelet-rich plasmapheresis (aPRP) may reduce the need for transfusions by preserving blood components. However, the impact of aPRP on postoperative blood loss and clinical outcomes in cardiovascular surgery remains controversial. This study aimed to examine the effects of aPRP on postoperative blood loss and recovery in patients undergoing heart valve surgery.
Methods: A total of 183 patients were divided into either aPRP or control groups. The aPRP group received aPRP before CPB, whereas the control group did not. The primary endpoint was postoperative bleeding between the groups. The secondary endpoints were postoperative bleeding risk factors and clinical outcome assessment. Logistic regression analysis with covariate adjustment was used to calculate these risk factors.
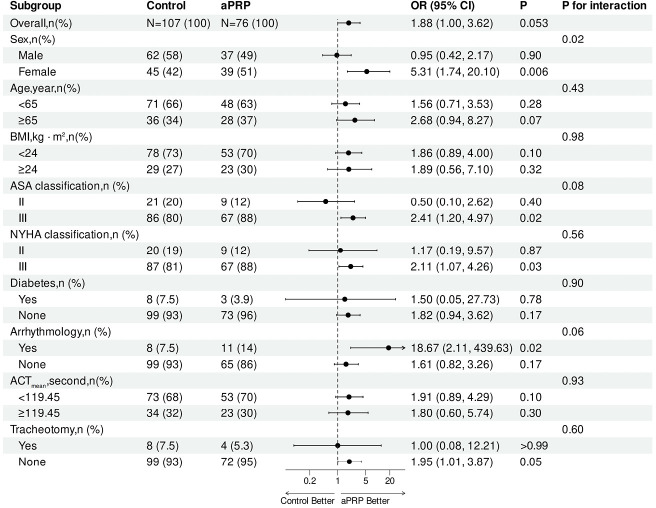
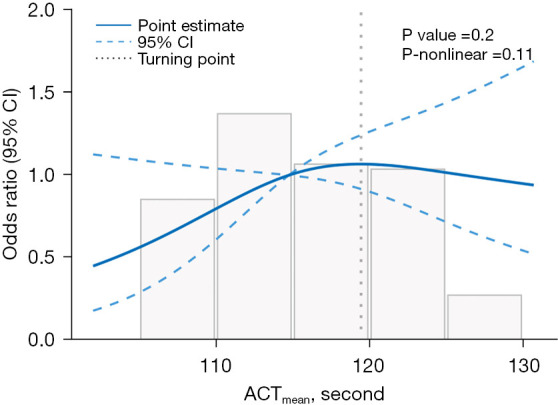
Results: A total of 76 patients (41.5%) in the aPRP group and 107 patients (58.5%) in the control group were included in the analysis. No significant difference was found in the occurrence of postoperative bleeding [odds ratio (OR) =0.53, 95% confidence interval (CI): 0.28-1.00, P=0.05], and the aPRP group had fewer complications than the controls (OR =0.28, 95% CI: 0.10-0.68, P=0.009). However, after adjusting for the New York Heart Association (NYHA) classification, diabetes, arrhythmology, mean activated clotting time (ACTmean), CPB, bleeding, thoracotomy, and body mass index (BMI), there was a significant difference in postoperative bleeding (adjusted OR =0.47, 95% CI: 0.22-0.98, P=0.04) and complications (adjusted OR =0.23, 95% CI: 0.07-0.64, P=0.008) between the two groups.
Conclusions: Preoperative aPRP can improve postoperative outcomes and reduce complications in patients undergoing heart valve surgery.
期刊介绍:
The Journal of Thoracic Disease (JTD, J Thorac Dis, pISSN: 2072-1439; eISSN: 2077-6624) was founded in Dec 2009, and indexed in PubMed in Dec 2011 and Science Citation Index SCI in Feb 2013. It is published quarterly (Dec 2009- Dec 2011), bimonthly (Jan 2012 - Dec 2013), monthly (Jan. 2014-) and openly distributed worldwide. JTD received its impact factor of 2.365 for the year 2016. JTD publishes manuscripts that describe new findings and provide current, practical information on the diagnosis and treatment of conditions related to thoracic disease. All the submission and reviewing are conducted electronically so that rapid review is assured.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


