{"title":"将重症血友病 A 患者从 emicizumab 预防治疗过渡到 valoctocogene roxaparvovec 基因治疗:真实世界的临床经验。","authors":"Robert Klamroth, Saskia Gottstein","doi":"10.1111/hae.15086","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor</p><p>Valoctocogene roxaparvovec is a gene therapy that has been approved for the treatment of adults with severe haemophilia A since 2022 in Europe and 2023 in the USA.<span><sup>1, 2</sup></span> It uses an adeno-associated virus serotype 5 to deliver a functional copy of the B-domain-deleted factor VIII (FVIII)-encoding gene, <i>F8</i>, to hepatocytes, via a single infusion, to allow long-term expression of endogenous FVIII and prevention of bleeding in adults with severe haemophilia A.<span><sup>3</sup></span></p><p>Emicizumab, a humanised, recombinant, bispecific monoclonal antibody, has been approved in the USA and Europe since 2018 as routine prophylaxis for patients with severe haemophilia A, regardless of FVIII inhibitor status.<span><sup>4-6</sup></span> Emicizumab is administered subcutaneously at a dose of 3 mg/kg once weekly for the first 4 weeks, followed by a maintenance dose of 1.5 mg/kg once every week, 3 mg/kg once every 2 weeks or 6 mg/kg once every 4 weeks.<span><sup>4</sup></span> It acts by mimicking the function of activated FVIII and has a half-life of approximately 28−34 days.<span><sup>7</sup></span></p><p>Whilst the availability of gene therapy for severe haemophilia A represents a significant therapeutic milestone, new therapies may pose challenges to physicians on how to practically implement them within a patient's current treatment regimen. One such topic, addressed in the July 2024 issue of <i>Haemophilia</i>, is how to transition patients from one therapy to another.<span><sup>8</sup></span> Agarwal et al. used pharmacokinetic simulations to determine best practice for maintaining haemostatic control whilst transitioning patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy. Bleeding risk was estimated at three approved emicizumab dosing regimens (once a week, once every 2 weeks and once every 4 weeks) across two transition scenarios: last dose of emicizumab given on the day of valoctocogene roxaparvovec infusion versus last dose of emicizumab administered 4 weeks post-infusion. Haemostatic control was maintained regardless of emicizumab dosing regimen or scenario, suggesting that several approaches can safely transition patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy in the clinic.</p><p>An algorithm was subsequently presented to guide the timing of emicizumab discontinuation when transitioning to gene therapy. The authors suggested that FVIII activity levels should be evaluated 4 weeks post-valoctocogene roxaparvovec infusion. If FVIII is ≥ 5 IU/dL at Week 4 and remains ≥ 5 IU/dL at Week 5, discontinuation of emicizumab can be considered. If FVIII activity is < 5 IU/dL at Week 4, prescribers should consider continuing emicizumab prophylaxis until two consecutive weekly measurements of ≥ 5 IU/dL are achieved.</p><p>Here, we present details of our real-world clinical experience of transitioning an adult male patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy without a washout period.</p><p>The patient initially managed his haemophilia with intravenous FVIII prophylaxis but switched to subcutaneous emicizumab (105 mg/week) in 2021. After switching to emicizumab, the frequency of the patient's bleeding events decreased; throughout his time on emicizumab, he experienced one spontaneous bleed in his left elbow and suspicion of several bleeds and microbleeds in his left wrist. The latter were successfully treated with single infusions of recombinant FVIII.</p><p>In 2023, following the approval of valoctocogene roxaparvovec for use in adults with severe haemophilia A in Germany,<span><sup>9</sup></span> the patient became interested in switching to gene therapy in the hope of more reliably preventing the bleeds in his elbow. Although he did not present with a ‛heavy bleeding’ phenotype, he had always been afraid of bleeds, monitoring signs and symptoms closely, and the bleeds in his elbow caused him concern. He also expressed a wish to move away from the burden of repeated and lifelong prophylactic injections. After carefully considering the benefits and risks (short term and long term), including the potential requirement to receive a reactive course of corticosteroids to potentially protect FVIII expression should he experience transaminitis, a shared decision between the patient and clinical team was reached to switch to gene therapy.</p><p>Ahead of the patient's valoctocogene roxaparvovec infusion, no changes were made to the dosing frequency of emicizumab. In June 2023, his blood emicizumab concentration was 77 µg/mL. Thus, a steady-state concentration of 77 µg/mL was assumed at the time of gene therapy administration. His FVIII levels were < 0.3% under emicizumab, as measured by the chromogenic substrate assay (CSA).</p><p>The patient discontinued emicizumab 3 days prior to infusion with valoctocogene roxaparvovec in November 2023. This approach was taken based on the fact that emicizumab has an elimination half-life of approximately 28 days, remaining at a protective level of 30 µg/mL in the body for at least 4 weeks upon cessation of treatment.<span><sup>7, 10</sup></span> In our case, the high FVIII levels (159−381 IU/dL) observed from 2 months post-valoctocogene roxaparvovec administration precluded reliable measurement of emicizumab levels.</p><p>There were no notable adverse events during the valoctocogene roxaparvovec infusion; administration was straightforward according to the prescribing information<span><sup>11</sup></span> and guidance provided by the manufacturer. The patient found the administration process convenient and tolerated the infusion well.</p><p>In the days following the infusion, the patient experienced mild nausea and fever; these were transient and resolved without intervention. Aspartate transaminase levels remained within the upper limits of normal following administration of valoctocogene roxaparvovec, whilst only mild elevations in alanine transaminase levels were observed from 2 months post-infusion (Figure 1). Thus, the use of corticosteroids was deemed unnecessary. FVIII levels were monitored weekly via CSA using bovine reagents; FVIII levels were < 0.7 IU/dL 5 days post-infusion, 1.5 IU/dL 12 days post-infusion, 12.7 IU/dL 19 days post-infusion and 14.4 IU/dL 1 month post-infusion.</p><p>Five months on from the infusion, the patient continues to do well. His FVIII activity levels range from 300 to 350 IU/dL by CSA (Figure 1), and no bleeding events have occurred. Furthermore, no thromboembolic events have been observed. Daily anticoagulation has not been administered, although prophylactic low molecular weight heparin has been prescribed for use in situations where blood clot risk is high (e.g., long-distance travel); the patient has been educated fully on the symptoms of thrombosis and thromboembolism.</p><p>In summary, transitioning a patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec without a washout period proved straightforward and well tolerated. Whilst the recently outlined algorithm by Agarwal et al. suggests evaluating FVIII levels 4 weeks after valoctocogene roxaparvovec dosing and discontinuing emicizumab only if FVIII levels are ≥ 5 IU/dL, we elected to stop emicizumab treatment immediately. This was guided by the wish of the patient, a low number of breakthrough bleeds under emicizumab, relatively high emicizumab levels before valoctocogene roxaparvovec dosing, and the knowledge that the long half-life of emicizumab ensures that therapeutic concentrations remain for several weeks after cessation. Therefore, our centre's clinical experience can provide clinicians with additional confidence when transitioning their patients who wish to gain the benefits of gene therapy from emicizumab prophylaxis to valoctocogene roxaparvovec.</p><p>Both authors were responsible for drafting the text, providing investigation results and critically revising for important intellectual content. Both authors also approved the final manuscript for publication.</p><p>RK has received honoraria and/or been a member of advisory committees for Bayer, BioMarin, Biotest, CSL Behring, Grifols, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Roche/Chugai, Sanofi, Sobi and Shire/Takeda. SG has received payment for lectures, consulting, travel expenses and congress fees from Bayer, BioMarin, Chugai/Roche, CSL Behring, Novo Nordisk, Sobi and Takeda.</p><p>This study was funded by BioMarin.</p><p>We have received written consent from our patient to publish his data anonymously. We thank him for allowing his data to be presented.</p>","PeriodicalId":12819,"journal":{"name":"Haemophilia","volume":"30 5","pages":"1247-1249"},"PeriodicalIF":3.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.15086","citationCount":"0","resultStr":"{\"title\":\"Transitioning patients with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy: Real-world clinical experience\",\"authors\":\"Robert Klamroth, Saskia Gottstein\",\"doi\":\"10.1111/hae.15086\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor</p><p>Valoctocogene roxaparvovec is a gene therapy that has been approved for the treatment of adults with severe haemophilia A since 2022 in Europe and 2023 in the USA.<span><sup>1, 2</sup></span> It uses an adeno-associated virus serotype 5 to deliver a functional copy of the B-domain-deleted factor VIII (FVIII)-encoding gene, <i>F8</i>, to hepatocytes, via a single infusion, to allow long-term expression of endogenous FVIII and prevention of bleeding in adults with severe haemophilia A.<span><sup>3</sup></span></p><p>Emicizumab, a humanised, recombinant, bispecific monoclonal antibody, has been approved in the USA and Europe since 2018 as routine prophylaxis for patients with severe haemophilia A, regardless of FVIII inhibitor status.<span><sup>4-6</sup></span> Emicizumab is administered subcutaneously at a dose of 3 mg/kg once weekly for the first 4 weeks, followed by a maintenance dose of 1.5 mg/kg once every week, 3 mg/kg once every 2 weeks or 6 mg/kg once every 4 weeks.<span><sup>4</sup></span> It acts by mimicking the function of activated FVIII and has a half-life of approximately 28−34 days.<span><sup>7</sup></span></p><p>Whilst the availability of gene therapy for severe haemophilia A represents a significant therapeutic milestone, new therapies may pose challenges to physicians on how to practically implement them within a patient's current treatment regimen. One such topic, addressed in the July 2024 issue of <i>Haemophilia</i>, is how to transition patients from one therapy to another.<span><sup>8</sup></span> Agarwal et al. used pharmacokinetic simulations to determine best practice for maintaining haemostatic control whilst transitioning patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy. Bleeding risk was estimated at three approved emicizumab dosing regimens (once a week, once every 2 weeks and once every 4 weeks) across two transition scenarios: last dose of emicizumab given on the day of valoctocogene roxaparvovec infusion versus last dose of emicizumab administered 4 weeks post-infusion. Haemostatic control was maintained regardless of emicizumab dosing regimen or scenario, suggesting that several approaches can safely transition patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy in the clinic.</p><p>An algorithm was subsequently presented to guide the timing of emicizumab discontinuation when transitioning to gene therapy. The authors suggested that FVIII activity levels should be evaluated 4 weeks post-valoctocogene roxaparvovec infusion. If FVIII is ≥ 5 IU/dL at Week 4 and remains ≥ 5 IU/dL at Week 5, discontinuation of emicizumab can be considered. If FVIII activity is < 5 IU/dL at Week 4, prescribers should consider continuing emicizumab prophylaxis until two consecutive weekly measurements of ≥ 5 IU/dL are achieved.</p><p>Here, we present details of our real-world clinical experience of transitioning an adult male patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy without a washout period.</p><p>The patient initially managed his haemophilia with intravenous FVIII prophylaxis but switched to subcutaneous emicizumab (105 mg/week) in 2021. After switching to emicizumab, the frequency of the patient's bleeding events decreased; throughout his time on emicizumab, he experienced one spontaneous bleed in his left elbow and suspicion of several bleeds and microbleeds in his left wrist. The latter were successfully treated with single infusions of recombinant FVIII.</p><p>In 2023, following the approval of valoctocogene roxaparvovec for use in adults with severe haemophilia A in Germany,<span><sup>9</sup></span> the patient became interested in switching to gene therapy in the hope of more reliably preventing the bleeds in his elbow. Although he did not present with a ‛heavy bleeding’ phenotype, he had always been afraid of bleeds, monitoring signs and symptoms closely, and the bleeds in his elbow caused him concern. He also expressed a wish to move away from the burden of repeated and lifelong prophylactic injections. After carefully considering the benefits and risks (short term and long term), including the potential requirement to receive a reactive course of corticosteroids to potentially protect FVIII expression should he experience transaminitis, a shared decision between the patient and clinical team was reached to switch to gene therapy.</p><p>Ahead of the patient's valoctocogene roxaparvovec infusion, no changes were made to the dosing frequency of emicizumab. In June 2023, his blood emicizumab concentration was 77 µg/mL. Thus, a steady-state concentration of 77 µg/mL was assumed at the time of gene therapy administration. His FVIII levels were < 0.3% under emicizumab, as measured by the chromogenic substrate assay (CSA).</p><p>The patient discontinued emicizumab 3 days prior to infusion with valoctocogene roxaparvovec in November 2023. This approach was taken based on the fact that emicizumab has an elimination half-life of approximately 28 days, remaining at a protective level of 30 µg/mL in the body for at least 4 weeks upon cessation of treatment.<span><sup>7, 10</sup></span> In our case, the high FVIII levels (159−381 IU/dL) observed from 2 months post-valoctocogene roxaparvovec administration precluded reliable measurement of emicizumab levels.</p><p>There were no notable adverse events during the valoctocogene roxaparvovec infusion; administration was straightforward according to the prescribing information<span><sup>11</sup></span> and guidance provided by the manufacturer. The patient found the administration process convenient and tolerated the infusion well.</p><p>In the days following the infusion, the patient experienced mild nausea and fever; these were transient and resolved without intervention. Aspartate transaminase levels remained within the upper limits of normal following administration of valoctocogene roxaparvovec, whilst only mild elevations in alanine transaminase levels were observed from 2 months post-infusion (Figure 1). Thus, the use of corticosteroids was deemed unnecessary. FVIII levels were monitored weekly via CSA using bovine reagents; FVIII levels were < 0.7 IU/dL 5 days post-infusion, 1.5 IU/dL 12 days post-infusion, 12.7 IU/dL 19 days post-infusion and 14.4 IU/dL 1 month post-infusion.</p><p>Five months on from the infusion, the patient continues to do well. His FVIII activity levels range from 300 to 350 IU/dL by CSA (Figure 1), and no bleeding events have occurred. Furthermore, no thromboembolic events have been observed. Daily anticoagulation has not been administered, although prophylactic low molecular weight heparin has been prescribed for use in situations where blood clot risk is high (e.g., long-distance travel); the patient has been educated fully on the symptoms of thrombosis and thromboembolism.</p><p>In summary, transitioning a patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec without a washout period proved straightforward and well tolerated. Whilst the recently outlined algorithm by Agarwal et al. suggests evaluating FVIII levels 4 weeks after valoctocogene roxaparvovec dosing and discontinuing emicizumab only if FVIII levels are ≥ 5 IU/dL, we elected to stop emicizumab treatment immediately. This was guided by the wish of the patient, a low number of breakthrough bleeds under emicizumab, relatively high emicizumab levels before valoctocogene roxaparvovec dosing, and the knowledge that the long half-life of emicizumab ensures that therapeutic concentrations remain for several weeks after cessation. Therefore, our centre's clinical experience can provide clinicians with additional confidence when transitioning their patients who wish to gain the benefits of gene therapy from emicizumab prophylaxis to valoctocogene roxaparvovec.</p><p>Both authors were responsible for drafting the text, providing investigation results and critically revising for important intellectual content. Both authors also approved the final manuscript for publication.</p><p>RK has received honoraria and/or been a member of advisory committees for Bayer, BioMarin, Biotest, CSL Behring, Grifols, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Roche/Chugai, Sanofi, Sobi and Shire/Takeda. SG has received payment for lectures, consulting, travel expenses and congress fees from Bayer, BioMarin, Chugai/Roche, CSL Behring, Novo Nordisk, Sobi and Takeda.</p><p>This study was funded by BioMarin.</p><p>We have received written consent from our patient to publish his data anonymously. We thank him for allowing his data to be presented.</p>\",\"PeriodicalId\":12819,\"journal\":{\"name\":\"Haemophilia\",\"volume\":\"30 5\",\"pages\":\"1247-1249\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.15086\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Haemophilia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/hae.15086\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Haemophilia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hae.15086","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Transitioning patients with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy: Real-world clinical experience
Dear Editor
Valoctocogene roxaparvovec is a gene therapy that has been approved for the treatment of adults with severe haemophilia A since 2022 in Europe and 2023 in the USA.1, 2 It uses an adeno-associated virus serotype 5 to deliver a functional copy of the B-domain-deleted factor VIII (FVIII)-encoding gene, F8, to hepatocytes, via a single infusion, to allow long-term expression of endogenous FVIII and prevention of bleeding in adults with severe haemophilia A.3
Emicizumab, a humanised, recombinant, bispecific monoclonal antibody, has been approved in the USA and Europe since 2018 as routine prophylaxis for patients with severe haemophilia A, regardless of FVIII inhibitor status.4-6 Emicizumab is administered subcutaneously at a dose of 3 mg/kg once weekly for the first 4 weeks, followed by a maintenance dose of 1.5 mg/kg once every week, 3 mg/kg once every 2 weeks or 6 mg/kg once every 4 weeks.4 It acts by mimicking the function of activated FVIII and has a half-life of approximately 28−34 days.7
Whilst the availability of gene therapy for severe haemophilia A represents a significant therapeutic milestone, new therapies may pose challenges to physicians on how to practically implement them within a patient's current treatment regimen. One such topic, addressed in the July 2024 issue of Haemophilia, is how to transition patients from one therapy to another.8 Agarwal et al. used pharmacokinetic simulations to determine best practice for maintaining haemostatic control whilst transitioning patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy. Bleeding risk was estimated at three approved emicizumab dosing regimens (once a week, once every 2 weeks and once every 4 weeks) across two transition scenarios: last dose of emicizumab given on the day of valoctocogene roxaparvovec infusion versus last dose of emicizumab administered 4 weeks post-infusion. Haemostatic control was maintained regardless of emicizumab dosing regimen or scenario, suggesting that several approaches can safely transition patients from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy in the clinic.
An algorithm was subsequently presented to guide the timing of emicizumab discontinuation when transitioning to gene therapy. The authors suggested that FVIII activity levels should be evaluated 4 weeks post-valoctocogene roxaparvovec infusion. If FVIII is ≥ 5 IU/dL at Week 4 and remains ≥ 5 IU/dL at Week 5, discontinuation of emicizumab can be considered. If FVIII activity is < 5 IU/dL at Week 4, prescribers should consider continuing emicizumab prophylaxis until two consecutive weekly measurements of ≥ 5 IU/dL are achieved.
Here, we present details of our real-world clinical experience of transitioning an adult male patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec gene therapy without a washout period.
The patient initially managed his haemophilia with intravenous FVIII prophylaxis but switched to subcutaneous emicizumab (105 mg/week) in 2021. After switching to emicizumab, the frequency of the patient's bleeding events decreased; throughout his time on emicizumab, he experienced one spontaneous bleed in his left elbow and suspicion of several bleeds and microbleeds in his left wrist. The latter were successfully treated with single infusions of recombinant FVIII.
In 2023, following the approval of valoctocogene roxaparvovec for use in adults with severe haemophilia A in Germany,9 the patient became interested in switching to gene therapy in the hope of more reliably preventing the bleeds in his elbow. Although he did not present with a ‛heavy bleeding’ phenotype, he had always been afraid of bleeds, monitoring signs and symptoms closely, and the bleeds in his elbow caused him concern. He also expressed a wish to move away from the burden of repeated and lifelong prophylactic injections. After carefully considering the benefits and risks (short term and long term), including the potential requirement to receive a reactive course of corticosteroids to potentially protect FVIII expression should he experience transaminitis, a shared decision between the patient and clinical team was reached to switch to gene therapy.
Ahead of the patient's valoctocogene roxaparvovec infusion, no changes were made to the dosing frequency of emicizumab. In June 2023, his blood emicizumab concentration was 77 µg/mL. Thus, a steady-state concentration of 77 µg/mL was assumed at the time of gene therapy administration. His FVIII levels were < 0.3% under emicizumab, as measured by the chromogenic substrate assay (CSA).
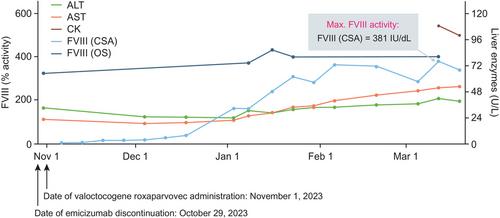
The patient discontinued emicizumab 3 days prior to infusion with valoctocogene roxaparvovec in November 2023. This approach was taken based on the fact that emicizumab has an elimination half-life of approximately 28 days, remaining at a protective level of 30 µg/mL in the body for at least 4 weeks upon cessation of treatment.7, 10 In our case, the high FVIII levels (159−381 IU/dL) observed from 2 months post-valoctocogene roxaparvovec administration precluded reliable measurement of emicizumab levels.
There were no notable adverse events during the valoctocogene roxaparvovec infusion; administration was straightforward according to the prescribing information11 and guidance provided by the manufacturer. The patient found the administration process convenient and tolerated the infusion well.
In the days following the infusion, the patient experienced mild nausea and fever; these were transient and resolved without intervention. Aspartate transaminase levels remained within the upper limits of normal following administration of valoctocogene roxaparvovec, whilst only mild elevations in alanine transaminase levels were observed from 2 months post-infusion (Figure 1). Thus, the use of corticosteroids was deemed unnecessary. FVIII levels were monitored weekly via CSA using bovine reagents; FVIII levels were < 0.7 IU/dL 5 days post-infusion, 1.5 IU/dL 12 days post-infusion, 12.7 IU/dL 19 days post-infusion and 14.4 IU/dL 1 month post-infusion.
Five months on from the infusion, the patient continues to do well. His FVIII activity levels range from 300 to 350 IU/dL by CSA (Figure 1), and no bleeding events have occurred. Furthermore, no thromboembolic events have been observed. Daily anticoagulation has not been administered, although prophylactic low molecular weight heparin has been prescribed for use in situations where blood clot risk is high (e.g., long-distance travel); the patient has been educated fully on the symptoms of thrombosis and thromboembolism.
In summary, transitioning a patient with severe haemophilia A from emicizumab prophylaxis to valoctocogene roxaparvovec without a washout period proved straightforward and well tolerated. Whilst the recently outlined algorithm by Agarwal et al. suggests evaluating FVIII levels 4 weeks after valoctocogene roxaparvovec dosing and discontinuing emicizumab only if FVIII levels are ≥ 5 IU/dL, we elected to stop emicizumab treatment immediately. This was guided by the wish of the patient, a low number of breakthrough bleeds under emicizumab, relatively high emicizumab levels before valoctocogene roxaparvovec dosing, and the knowledge that the long half-life of emicizumab ensures that therapeutic concentrations remain for several weeks after cessation. Therefore, our centre's clinical experience can provide clinicians with additional confidence when transitioning their patients who wish to gain the benefits of gene therapy from emicizumab prophylaxis to valoctocogene roxaparvovec.
Both authors were responsible for drafting the text, providing investigation results and critically revising for important intellectual content. Both authors also approved the final manuscript for publication.
RK has received honoraria and/or been a member of advisory committees for Bayer, BioMarin, Biotest, CSL Behring, Grifols, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Roche/Chugai, Sanofi, Sobi and Shire/Takeda. SG has received payment for lectures, consulting, travel expenses and congress fees from Bayer, BioMarin, Chugai/Roche, CSL Behring, Novo Nordisk, Sobi and Takeda.
This study was funded by BioMarin.
We have received written consent from our patient to publish his data anonymously. We thank him for allowing his data to be presented.
期刊介绍:
Haemophilia is an international journal dedicated to the exchange of information regarding the comprehensive care of haemophilia. The Journal contains review articles, original scientific papers and case reports related to haemophilia care, with frequent supplements. Subjects covered include:
clotting factor deficiencies, both inherited and acquired: haemophilia A, B, von Willebrand''s disease, deficiencies of factor V, VII, X and XI
replacement therapy for clotting factor deficiencies
component therapy in the developing world
transfusion transmitted disease
haemophilia care and paediatrics, orthopaedics, gynaecology and obstetrics
nursing
laboratory diagnosis
carrier detection
psycho-social concerns
economic issues
audit
inherited platelet disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


