Zouheir Ibrahim Bitar, Ossama Maadarani, Hussien Dashti, Abdullah Alenezi, Khaled Almerri
{"title":"对重度主动脉瓣狭窄患者超声 B 线、心脏组织多普勒信号和左心室舒张末压之间相关性的前瞻性分析。","authors":"Zouheir Ibrahim Bitar, Ossama Maadarani, Hussien Dashti, Abdullah Alenezi, Khaled Almerri","doi":"10.1186/s44156-024-00055-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The development of heart failure is a turning point in the natural course of aortic stenosis (AS). Pulmonary oedema and elevated left ventricular pressure (LVP) are cardinal features of heart failure. Evaluating pulmonary oedema by lung ultrasound involves taking the upper hand with a bedside noninvasive tool that may reflect LVP.</p><p><strong>Aim: </strong>We sought to assess the correlation between sonographic pulmonary congestion, invasive LV pre-A pressure, and echocardiographic LV end-diastolic pressure (LVEDP) in symptomatic AS patients receiving transcatheter aortic valve replacement.</p><p><strong>Methods: </strong>Forty-eight consecutive patients with severe AS and planned transcatheter aortic valve implantation (TAVI) were enrolled. LVEDP was estimated to be normal or elevated using the ASE/EACVI algorithm and transmitral Doppler indices, the E/A ratio, the E/e', and the left atrial volume index. Invasive LV pre-A pressure was used as a reference, with > 12 mm Hg defined as elevated.</p><p><strong>Results: </strong>Forty-eight patients (25 women (52%), mean age 75 years, standard deviation (SD) ± 7.7 years) were enrolled in the study. We detected severe B-lines (≥ 30) in 13 (27%) patients and moderate B-lines (15-30) in 33 (68.6%) patients. The number of B-lines increased significantly with the severity of New York Heart Association (NYHA) functional classes (Fig. 1). The B-line count was 14 ± 13 in NYHA class I patients, 20 ± 20 in class II patients, and 44 ± 35 in class III patients (p < 0.05, rho = 0.384). The number of B-lines was correlated with the E/E' ratio (R = 0.664, p < 0.0001) and the proBNP level (R = 0. 882, p < 0.008). We found no significant correlation with the LVEDP or LVEF. The LVEDP correlated well with the E/E' ratio (R = 0.491, p < 0.001) but not at all with E/A, DT, or LAVI. All patients had an elevated LVEDP > 12, with a mean pressure of 26 mmHg, a minimum of 13 mmHg, and a maximum of 45 mmHg, with an SD of 7.85.</p><p><strong>Conclusion: </strong>Assessing lung ultrasonic B-lines is a straightforward and practical approach to identifying pulmonary oedema in AS patients. The number of B-lines correlated with the E/E' ratio and the functional status of patients but did not correlate with invasive LVEDP or LVEF. All patients had elevated LVEDP that correlated with E/E'.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"11 1","pages":"21"},"PeriodicalIF":2.4000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11318176/pdf/","citationCount":"0","resultStr":"{\"title\":\"A prospective analysis of the correlation between ultrasonic B-lines, cardiac tissue doppler signals and left ventricular end-diastolic pressure in patients with severe aortic stenosis.\",\"authors\":\"Zouheir Ibrahim Bitar, Ossama Maadarani, Hussien Dashti, Abdullah Alenezi, Khaled Almerri\",\"doi\":\"10.1186/s44156-024-00055-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The development of heart failure is a turning point in the natural course of aortic stenosis (AS). Pulmonary oedema and elevated left ventricular pressure (LVP) are cardinal features of heart failure. Evaluating pulmonary oedema by lung ultrasound involves taking the upper hand with a bedside noninvasive tool that may reflect LVP.</p><p><strong>Aim: </strong>We sought to assess the correlation between sonographic pulmonary congestion, invasive LV pre-A pressure, and echocardiographic LV end-diastolic pressure (LVEDP) in symptomatic AS patients receiving transcatheter aortic valve replacement.</p><p><strong>Methods: </strong>Forty-eight consecutive patients with severe AS and planned transcatheter aortic valve implantation (TAVI) were enrolled. LVEDP was estimated to be normal or elevated using the ASE/EACVI algorithm and transmitral Doppler indices, the E/A ratio, the E/e', and the left atrial volume index. Invasive LV pre-A pressure was used as a reference, with > 12 mm Hg defined as elevated.</p><p><strong>Results: </strong>Forty-eight patients (25 women (52%), mean age 75 years, standard deviation (SD) ± 7.7 years) were enrolled in the study. We detected severe B-lines (≥ 30) in 13 (27%) patients and moderate B-lines (15-30) in 33 (68.6%) patients. The number of B-lines increased significantly with the severity of New York Heart Association (NYHA) functional classes (Fig. 1). The B-line count was 14 ± 13 in NYHA class I patients, 20 ± 20 in class II patients, and 44 ± 35 in class III patients (p < 0.05, rho = 0.384). The number of B-lines was correlated with the E/E' ratio (R = 0.664, p < 0.0001) and the proBNP level (R = 0. 882, p < 0.008). We found no significant correlation with the LVEDP or LVEF. The LVEDP correlated well with the E/E' ratio (R = 0.491, p < 0.001) but not at all with E/A, DT, or LAVI. All patients had an elevated LVEDP > 12, with a mean pressure of 26 mmHg, a minimum of 13 mmHg, and a maximum of 45 mmHg, with an SD of 7.85.</p><p><strong>Conclusion: </strong>Assessing lung ultrasonic B-lines is a straightforward and practical approach to identifying pulmonary oedema in AS patients. The number of B-lines correlated with the E/E' ratio and the functional status of patients but did not correlate with invasive LVEDP or LVEF. All patients had elevated LVEDP that correlated with E/E'.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"11 1\",\"pages\":\"21\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11318176/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-024-00055-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-024-00055-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
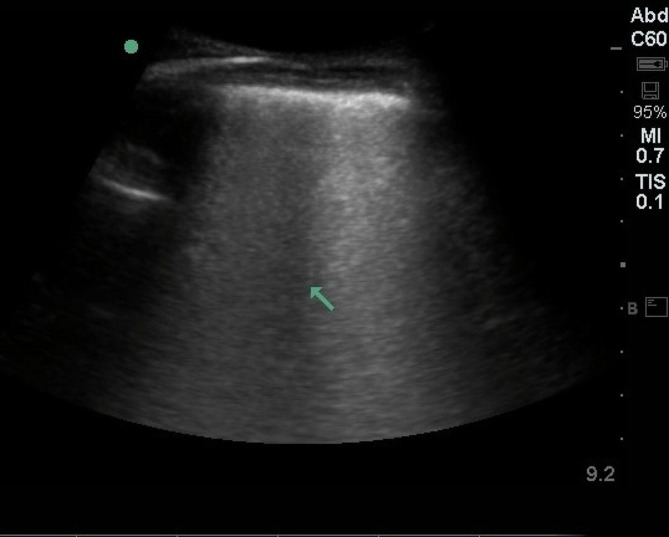
背景:心力衰竭的发生是主动脉瓣狭窄(AS)自然病程的转折点。肺水肿和左心室压力(LVP)升高是心力衰竭的主要特征。目的:我们试图评估接受经导管主动脉瓣置换术的无症状AS患者声像图肺部充血、有创左心室前A压和超声心动图左心室舒张末期压(LVEDP)之间的相关性:方法: 连续纳入48例计划接受经导管主动脉瓣植入术(TAVI)的重度AS患者。使用 ASE/EACVI 算法和透射性多普勒指数、E/A 比值、E/e' 和左心房容积指数估计 LVEDP 正常或升高。将有创左心室前A压作为参考,大于12毫米汞柱定义为升高:48名患者(25名女性(52%),平均年龄75岁,标准差(SD)±7.7岁)参与了研究。我们在 13 名(27%)患者中检测到重度 B 线(≥ 30),在 33 名(68.6%)患者中检测到中度 B 线(15-30)。随着纽约心脏协会(NYHA)功能分级的严重程度不同,B 线的数量也明显增加(图 1)。NYHA I 级患者的 B 线数为 14 ± 13,II 级患者为 20 ± 20,III 级患者为 44 ± 35(P 12),平均压力为 26 mmHg,最低压力为 13 mmHg,最高压力为 45 mmHg,SD 为 7.85:评估肺超声 B 线是鉴别强直性脊柱炎患者肺水肿的一种简单实用的方法。B线的数量与E/E'比值和患者的功能状态相关,但与有创LVEDP或LVEF无关。所有患者的 LVEDP 均升高,且与 E/E' 相关。
A prospective analysis of the correlation between ultrasonic B-lines, cardiac tissue doppler signals and left ventricular end-diastolic pressure in patients with severe aortic stenosis.
Background: The development of heart failure is a turning point in the natural course of aortic stenosis (AS). Pulmonary oedema and elevated left ventricular pressure (LVP) are cardinal features of heart failure. Evaluating pulmonary oedema by lung ultrasound involves taking the upper hand with a bedside noninvasive tool that may reflect LVP.
Aim: We sought to assess the correlation between sonographic pulmonary congestion, invasive LV pre-A pressure, and echocardiographic LV end-diastolic pressure (LVEDP) in symptomatic AS patients receiving transcatheter aortic valve replacement.
Methods: Forty-eight consecutive patients with severe AS and planned transcatheter aortic valve implantation (TAVI) were enrolled. LVEDP was estimated to be normal or elevated using the ASE/EACVI algorithm and transmitral Doppler indices, the E/A ratio, the E/e', and the left atrial volume index. Invasive LV pre-A pressure was used as a reference, with > 12 mm Hg defined as elevated.
Results: Forty-eight patients (25 women (52%), mean age 75 years, standard deviation (SD) ± 7.7 years) were enrolled in the study. We detected severe B-lines (≥ 30) in 13 (27%) patients and moderate B-lines (15-30) in 33 (68.6%) patients. The number of B-lines increased significantly with the severity of New York Heart Association (NYHA) functional classes (Fig. 1). The B-line count was 14 ± 13 in NYHA class I patients, 20 ± 20 in class II patients, and 44 ± 35 in class III patients (p < 0.05, rho = 0.384). The number of B-lines was correlated with the E/E' ratio (R = 0.664, p < 0.0001) and the proBNP level (R = 0. 882, p < 0.008). We found no significant correlation with the LVEDP or LVEF. The LVEDP correlated well with the E/E' ratio (R = 0.491, p < 0.001) but not at all with E/A, DT, or LAVI. All patients had an elevated LVEDP > 12, with a mean pressure of 26 mmHg, a minimum of 13 mmHg, and a maximum of 45 mmHg, with an SD of 7.85.
Conclusion: Assessing lung ultrasonic B-lines is a straightforward and practical approach to identifying pulmonary oedema in AS patients. The number of B-lines correlated with the E/E' ratio and the functional status of patients but did not correlate with invasive LVEDP or LVEF. All patients had elevated LVEDP that correlated with E/E'.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


