{"title":"线粒体心肌病和低心功能患者经皮二尖瓣修复术的麻醉管理:病例报告。","authors":"Koichiro Tashima, Masakiyo Hayashi, Takafumi Oyoshi, Jo Uemura, Shinnosuke Korematsu, Naoyuki Hirata","doi":"10.1186/s40981-024-00734-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mitochondrial cardiomyopathy occurs when impaired mitochondrial energy production leads to myocardial dysfunction. Anesthetic management in such cases is challenging due to risks of circulatory depression associated with anesthesia and mitochondrial dysfunction induced by anesthetics. Although there are reports of anesthetic management for patients with mitochondrial diseases, there are few reports specifically addressing cardiac anesthesia for patients with mitochondrial cardiomyopathy. We present a case where percutaneous mitral valve repair with MitraClip™ was successfully performed under remimazolam anesthesia in a patient with mitochondrial cardiomyopathy who developed functional mitral valve regurgitation due to low cardiac function and cardiomegaly.</p><p><strong>Case presentation: </strong>A 57-year-old woman was diagnosed with chronic cardiac failure, with a 10-year history of dilated cardiomyopathy. She was diagnosed with mitochondrial cardiomyopathy 8 years ago. Over the past 2 years, her cardiac failure worsened, and mitral valve regurgitation gradually developed. Surgical intervention was considered but deemed too risky due to her low cardiac function, with an ejection fraction of 26%. Therefore, percutaneous MitraClip™ implantation was selected. After securing radial artery and central venous catheterization under sedation with dexmedetomidine, anesthesia was induced with a low dose of remimazolam 4 mg/kg/h. Anesthesia was maintained with remimazolam 0.35-1.0 mg/kg/h and remifentanil 0.1 μg/kg/min. Noradrenaline and dobutamine were administered intraoperatively, and the procedure was completed successfully without circulatory collapse. The patient recovered smoothly from anesthesia and experienced no complications. She was discharged on the eighth day after surgery.</p><p><strong>Conclusion: </strong>Anesthesia management with remimazolam appears to be a safe and effective for MitraClip™ implantation in patients with mitochondrial cardiomyopathy.</p>","PeriodicalId":14635,"journal":{"name":"JA Clinical Reports","volume":"10 1","pages":"49"},"PeriodicalIF":1.0000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11310374/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anesthesia management for percutaneous mitral valve repair in a patient with mitochondrial cardiomyopathy and low cardiac function: a case report.\",\"authors\":\"Koichiro Tashima, Masakiyo Hayashi, Takafumi Oyoshi, Jo Uemura, Shinnosuke Korematsu, Naoyuki Hirata\",\"doi\":\"10.1186/s40981-024-00734-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Mitochondrial cardiomyopathy occurs when impaired mitochondrial energy production leads to myocardial dysfunction. Anesthetic management in such cases is challenging due to risks of circulatory depression associated with anesthesia and mitochondrial dysfunction induced by anesthetics. Although there are reports of anesthetic management for patients with mitochondrial diseases, there are few reports specifically addressing cardiac anesthesia for patients with mitochondrial cardiomyopathy. We present a case where percutaneous mitral valve repair with MitraClip™ was successfully performed under remimazolam anesthesia in a patient with mitochondrial cardiomyopathy who developed functional mitral valve regurgitation due to low cardiac function and cardiomegaly.</p><p><strong>Case presentation: </strong>A 57-year-old woman was diagnosed with chronic cardiac failure, with a 10-year history of dilated cardiomyopathy. She was diagnosed with mitochondrial cardiomyopathy 8 years ago. Over the past 2 years, her cardiac failure worsened, and mitral valve regurgitation gradually developed. Surgical intervention was considered but deemed too risky due to her low cardiac function, with an ejection fraction of 26%. Therefore, percutaneous MitraClip™ implantation was selected. After securing radial artery and central venous catheterization under sedation with dexmedetomidine, anesthesia was induced with a low dose of remimazolam 4 mg/kg/h. Anesthesia was maintained with remimazolam 0.35-1.0 mg/kg/h and remifentanil 0.1 μg/kg/min. Noradrenaline and dobutamine were administered intraoperatively, and the procedure was completed successfully without circulatory collapse. The patient recovered smoothly from anesthesia and experienced no complications. She was discharged on the eighth day after surgery.</p><p><strong>Conclusion: </strong>Anesthesia management with remimazolam appears to be a safe and effective for MitraClip™ implantation in patients with mitochondrial cardiomyopathy.</p>\",\"PeriodicalId\":14635,\"journal\":{\"name\":\"JA Clinical Reports\",\"volume\":\"10 1\",\"pages\":\"49\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11310374/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JA Clinical Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40981-024-00734-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JA Clinical Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40981-024-00734-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Anesthesia management for percutaneous mitral valve repair in a patient with mitochondrial cardiomyopathy and low cardiac function: a case report.
Background: Mitochondrial cardiomyopathy occurs when impaired mitochondrial energy production leads to myocardial dysfunction. Anesthetic management in such cases is challenging due to risks of circulatory depression associated with anesthesia and mitochondrial dysfunction induced by anesthetics. Although there are reports of anesthetic management for patients with mitochondrial diseases, there are few reports specifically addressing cardiac anesthesia for patients with mitochondrial cardiomyopathy. We present a case where percutaneous mitral valve repair with MitraClip™ was successfully performed under remimazolam anesthesia in a patient with mitochondrial cardiomyopathy who developed functional mitral valve regurgitation due to low cardiac function and cardiomegaly.
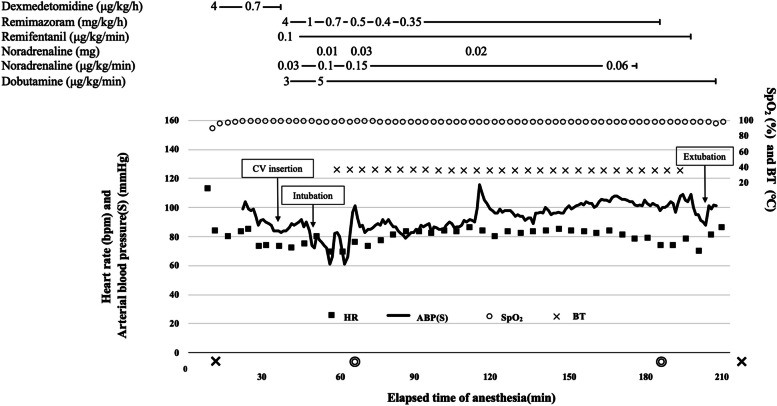
Case presentation: A 57-year-old woman was diagnosed with chronic cardiac failure, with a 10-year history of dilated cardiomyopathy. She was diagnosed with mitochondrial cardiomyopathy 8 years ago. Over the past 2 years, her cardiac failure worsened, and mitral valve regurgitation gradually developed. Surgical intervention was considered but deemed too risky due to her low cardiac function, with an ejection fraction of 26%. Therefore, percutaneous MitraClip™ implantation was selected. After securing radial artery and central venous catheterization under sedation with dexmedetomidine, anesthesia was induced with a low dose of remimazolam 4 mg/kg/h. Anesthesia was maintained with remimazolam 0.35-1.0 mg/kg/h and remifentanil 0.1 μg/kg/min. Noradrenaline and dobutamine were administered intraoperatively, and the procedure was completed successfully without circulatory collapse. The patient recovered smoothly from anesthesia and experienced no complications. She was discharged on the eighth day after surgery.
Conclusion: Anesthesia management with remimazolam appears to be a safe and effective for MitraClip™ implantation in patients with mitochondrial cardiomyopathy.
期刊介绍:
JA Clinical Reports is a companion journal to the Journal of Anesthesia (JA), the official journal of the Japanese Society of Anesthesiologists (JSA). This journal is an open access, peer-reviewed, online journal related to clinical anesthesia practices such as anesthesia management, pain management and intensive care. Case reports are very important articles from the viewpoint of education and the cultivation of scientific thinking in the field of anesthesia. However, submissions of anesthesia research and clinical reports from Japan are notably decreasing in major anesthesia journals. Therefore, the JSA has decided to launch a new journal, JA Clinical Reports, to encourage JSA members, particularly junior Japanese anesthesiologists, to publish papers in English language.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


