Jenna N. Whitrock, Stephanie Sisak, Catherine G. Pratt, Aaron M. Delman, Adam D. Price, Koffi Wima, Shimul A. Shah, Ralph Cutler Quillin III
{"title":"现代肝移植中的初级团队与局部恢复:器官共享联合网络数据库的全国性分析。","authors":"Jenna N. Whitrock, Stephanie Sisak, Catherine G. Pratt, Aaron M. Delman, Adam D. Price, Koffi Wima, Shimul A. Shah, Ralph Cutler Quillin III","doi":"10.1111/ctr.15418","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The implementation of acuity circles (AC) in 2020 and the COVID-19 pandemic increased the use of local surgeons to recover livers for transplant; however, the impact on liver transplant (LT) outcomes is unknown.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Deceased donor adult LT recipients from the UNOS database were identified. Recipients were grouped by donor surgeon: local versus primary recovery. Patient and graft survival as well as trends in local recovery in the 2 years pre-AC and post-AC were assessed.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The utilization of local recovery in LT increased from 22.3% to 37.9% post-AC (<i>p</i> < 0.01). LTs with local recovery had longer cold ischemia times (6.5 h [5.4–7.8] vs. 5.3 h [4.4–6.5], <i>p</i> < 0.01) and traveled further (210 miles [89–373] vs. 73 miles [11–196], <i>p</i> < 0.01) than those using primary recovery. Multivariate analyses revealed no differences in patient or graft survival between local and primary recovery, and between OPO and local surgeon. There was no difference in survival when comparing simultaneous liver–kidney, donation after circulatory death, MELD ≥ 30, or redo-LT by recovery team. Recovery and utilization rates were also noted to be higher post-AC (51.4% vs. 48.6% pre-AC, <i>p</i> < 0.01) as well as when OPO surgeons recovered the allografts (72.5% vs. 66.0%, <i>p</i> < 0.01).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Nearly 40% of LTs are performed using local recovery, and utilization rates and trends continue to change with changing organ-sharing paradigms such as AC. This practice appears safe with outcomes similar to recovery by the primary team in appropriately selected recipients and may lead to increased access and the ability to transplant more livers.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 8","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15418","citationCount":"0","resultStr":"{\"title\":\"Primary Team Versus Local Recovery in Liver Transplantation in the Modern Era: A National Analysis of the United Network for Organ Sharing Database\",\"authors\":\"Jenna N. Whitrock, Stephanie Sisak, Catherine G. Pratt, Aaron M. Delman, Adam D. Price, Koffi Wima, Shimul A. Shah, Ralph Cutler Quillin III\",\"doi\":\"10.1111/ctr.15418\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The implementation of acuity circles (AC) in 2020 and the COVID-19 pandemic increased the use of local surgeons to recover livers for transplant; however, the impact on liver transplant (LT) outcomes is unknown.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Deceased donor adult LT recipients from the UNOS database were identified. Recipients were grouped by donor surgeon: local versus primary recovery. Patient and graft survival as well as trends in local recovery in the 2 years pre-AC and post-AC were assessed.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The utilization of local recovery in LT increased from 22.3% to 37.9% post-AC (<i>p</i> < 0.01). LTs with local recovery had longer cold ischemia times (6.5 h [5.4–7.8] vs. 5.3 h [4.4–6.5], <i>p</i> < 0.01) and traveled further (210 miles [89–373] vs. 73 miles [11–196], <i>p</i> < 0.01) than those using primary recovery. Multivariate analyses revealed no differences in patient or graft survival between local and primary recovery, and between OPO and local surgeon. There was no difference in survival when comparing simultaneous liver–kidney, donation after circulatory death, MELD ≥ 30, or redo-LT by recovery team. Recovery and utilization rates were also noted to be higher post-AC (51.4% vs. 48.6% pre-AC, <i>p</i> < 0.01) as well as when OPO surgeons recovered the allografts (72.5% vs. 66.0%, <i>p</i> < 0.01).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Nearly 40% of LTs are performed using local recovery, and utilization rates and trends continue to change with changing organ-sharing paradigms such as AC. This practice appears safe with outcomes similar to recovery by the primary team in appropriately selected recipients and may lead to increased access and the ability to transplant more livers.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":\"38 8\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15418\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15418\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15418","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
背景:2020 年实施的敏锐圈(AC)和 COVID-19 大流行增加了当地外科医生回收肝脏用于移植的使用;然而,对肝移植(LT)结果的影响尚不清楚:方法:从 UNOS 数据库中确定了已故捐献者的成人 LT 受体。方法:对 UNOS 数据库中的死亡供体成人肝移植受者进行了鉴定,并根据供体外科医生进行了分组:本地外科医生和主要回收外科医生。评估了患者和移植物的存活率,以及器官移植前和器官移植后两年内局部复苏的趋势:结果:LT术中局部复苏的使用率从22.3%上升到AC术后的37.9%(p 结论:近40%的LT术使用局部复苏:近40%的LT使用局部复苏,随着器官共享模式(如AC)的改变,使用率和趋势也在不断变化。在适当选择受体的情况下,这种做法似乎是安全的,其结果与主治团队的复苏相似,可能会增加移植机会和移植更多肝脏的能力。
Primary Team Versus Local Recovery in Liver Transplantation in the Modern Era: A National Analysis of the United Network for Organ Sharing Database
Background
The implementation of acuity circles (AC) in 2020 and the COVID-19 pandemic increased the use of local surgeons to recover livers for transplant; however, the impact on liver transplant (LT) outcomes is unknown.
Methods
Deceased donor adult LT recipients from the UNOS database were identified. Recipients were grouped by donor surgeon: local versus primary recovery. Patient and graft survival as well as trends in local recovery in the 2 years pre-AC and post-AC were assessed.
Results
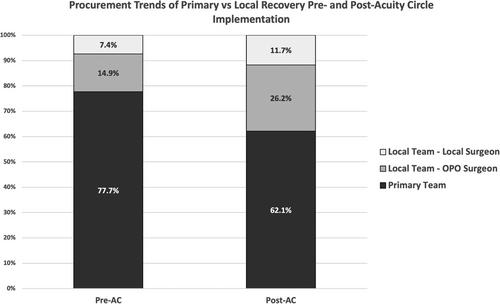
The utilization of local recovery in LT increased from 22.3% to 37.9% post-AC (p < 0.01). LTs with local recovery had longer cold ischemia times (6.5 h [5.4–7.8] vs. 5.3 h [4.4–6.5], p < 0.01) and traveled further (210 miles [89–373] vs. 73 miles [11–196], p < 0.01) than those using primary recovery. Multivariate analyses revealed no differences in patient or graft survival between local and primary recovery, and between OPO and local surgeon. There was no difference in survival when comparing simultaneous liver–kidney, donation after circulatory death, MELD ≥ 30, or redo-LT by recovery team. Recovery and utilization rates were also noted to be higher post-AC (51.4% vs. 48.6% pre-AC, p < 0.01) as well as when OPO surgeons recovered the allografts (72.5% vs. 66.0%, p < 0.01).
Conclusion
Nearly 40% of LTs are performed using local recovery, and utilization rates and trends continue to change with changing organ-sharing paradigms such as AC. This practice appears safe with outcomes similar to recovery by the primary team in appropriately selected recipients and may lead to increased access and the ability to transplant more livers.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


