Shao-Yang Zhang, Chang-Li Li, Jian Yin, Meng Jiang, Xiao-Feng Yang
{"title":"创伤性脑损伤的血压变异性和预后意义:eICU-CRD 数据库分析。","authors":"Shao-Yang Zhang, Chang-Li Li, Jian Yin, Meng Jiang, Xiao-Feng Yang","doi":"10.1186/s12873-024-01054-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preliminary evidence demonstrates that visit-to-visit systolic blood pressure (SBP) variability is a prognostic factor of TBI. However, literature regarding the impact of initial blood pressure management on the outcomes of TBI patients is limited. We aimed to further validate the clinical significance of BPV on the prognostic outcomes of patients with TBI.</p><p><strong>Methods: </strong>We performed the analysis by using individual patient-level data acquired from the eICU-CRD, which collected 200,859 ICU admissions of 139,367 patients in 2014 and 2015 from 208 US hospitals. Adult patients with traumatic intraparenchymal hemorrhage or contusion were included. The primary outcome was in-hospital mortality and the secondary outcome was discharge-home rate. Blood pressure variability (BPV) was calculated according to standard criteria: at least six measurements were taken in the first 24 h (hyperacute group) and 36 over days 2-7 (acute group). We estimated the associations between BPV and outcomes with logistic and proportional odds regression models. The key parameter for BPV was standard deviation (SD) of SBP, categorized into quintiles. We also calculated the average real variability (ARV), as well as maximum, minimum, and mean SBP for comparison in our analysis.</p><p><strong>Results: </strong>We studied 1486 patients in the hyperacute group and 857 in the acute group. SD of SBP had a significant association with the in-hospital mortality for both the hyperacute group (highest quintile adjusted OR 2.28 95% CI 1.18-4.42; p<sub>trend</sub><0.001) and the acute group (highest quintile adjusted OR 2.17, 95% CI 1.08-4.36; p<sub>trend</sub><0.001). The strongest predictors of primary outcome were SD of SBP in the hyperacute phase and minimum SBP in the acute phase. Associations were similar for the discharge-home rate (for the hyperacute group, highest quintile adjusted OR 0.58, 95% CI 0.37-0.89; p<sub>trend</sub><0.001; for the acute group OR 0.55, 95% CI 0.32-0.95; p<sub>trend</sub><0.001).</p><p><strong>Conclusion: </strong>Systolic BPV seems to predict a poor outcome in patients with TBI. The benefits of early treatment to maintain appropriate SBP level might be enhanced by smooth and sustained control.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"24 1","pages":"141"},"PeriodicalIF":2.3000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11305040/pdf/","citationCount":"0","resultStr":"{\"title\":\"Blood pressure variability and prognostic significance in traumatic brain injury: analysis of the eICU-CRD database.\",\"authors\":\"Shao-Yang Zhang, Chang-Li Li, Jian Yin, Meng Jiang, Xiao-Feng Yang\",\"doi\":\"10.1186/s12873-024-01054-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Preliminary evidence demonstrates that visit-to-visit systolic blood pressure (SBP) variability is a prognostic factor of TBI. However, literature regarding the impact of initial blood pressure management on the outcomes of TBI patients is limited. We aimed to further validate the clinical significance of BPV on the prognostic outcomes of patients with TBI.</p><p><strong>Methods: </strong>We performed the analysis by using individual patient-level data acquired from the eICU-CRD, which collected 200,859 ICU admissions of 139,367 patients in 2014 and 2015 from 208 US hospitals. Adult patients with traumatic intraparenchymal hemorrhage or contusion were included. The primary outcome was in-hospital mortality and the secondary outcome was discharge-home rate. Blood pressure variability (BPV) was calculated according to standard criteria: at least six measurements were taken in the first 24 h (hyperacute group) and 36 over days 2-7 (acute group). We estimated the associations between BPV and outcomes with logistic and proportional odds regression models. The key parameter for BPV was standard deviation (SD) of SBP, categorized into quintiles. We also calculated the average real variability (ARV), as well as maximum, minimum, and mean SBP for comparison in our analysis.</p><p><strong>Results: </strong>We studied 1486 patients in the hyperacute group and 857 in the acute group. SD of SBP had a significant association with the in-hospital mortality for both the hyperacute group (highest quintile adjusted OR 2.28 95% CI 1.18-4.42; p<sub>trend</sub><0.001) and the acute group (highest quintile adjusted OR 2.17, 95% CI 1.08-4.36; p<sub>trend</sub><0.001). The strongest predictors of primary outcome were SD of SBP in the hyperacute phase and minimum SBP in the acute phase. Associations were similar for the discharge-home rate (for the hyperacute group, highest quintile adjusted OR 0.58, 95% CI 0.37-0.89; p<sub>trend</sub><0.001; for the acute group OR 0.55, 95% CI 0.32-0.95; p<sub>trend</sub><0.001).</p><p><strong>Conclusion: </strong>Systolic BPV seems to predict a poor outcome in patients with TBI. The benefits of early treatment to maintain appropriate SBP level might be enhanced by smooth and sustained control.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"24 1\",\"pages\":\"141\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11305040/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-024-01054-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-024-01054-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Blood pressure variability and prognostic significance in traumatic brain injury: analysis of the eICU-CRD database.
Background: Preliminary evidence demonstrates that visit-to-visit systolic blood pressure (SBP) variability is a prognostic factor of TBI. However, literature regarding the impact of initial blood pressure management on the outcomes of TBI patients is limited. We aimed to further validate the clinical significance of BPV on the prognostic outcomes of patients with TBI.
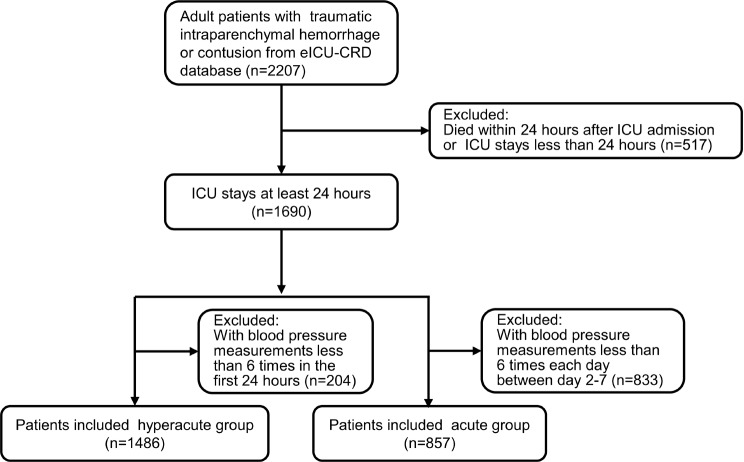
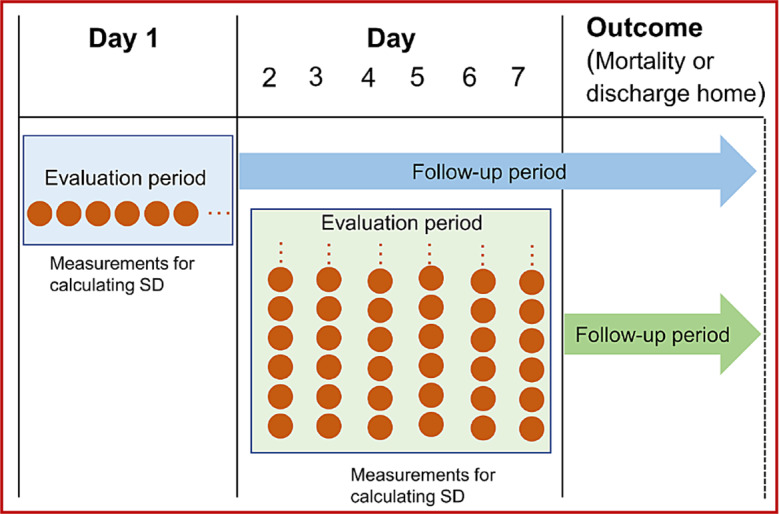
Methods: We performed the analysis by using individual patient-level data acquired from the eICU-CRD, which collected 200,859 ICU admissions of 139,367 patients in 2014 and 2015 from 208 US hospitals. Adult patients with traumatic intraparenchymal hemorrhage or contusion were included. The primary outcome was in-hospital mortality and the secondary outcome was discharge-home rate. Blood pressure variability (BPV) was calculated according to standard criteria: at least six measurements were taken in the first 24 h (hyperacute group) and 36 over days 2-7 (acute group). We estimated the associations between BPV and outcomes with logistic and proportional odds regression models. The key parameter for BPV was standard deviation (SD) of SBP, categorized into quintiles. We also calculated the average real variability (ARV), as well as maximum, minimum, and mean SBP for comparison in our analysis.
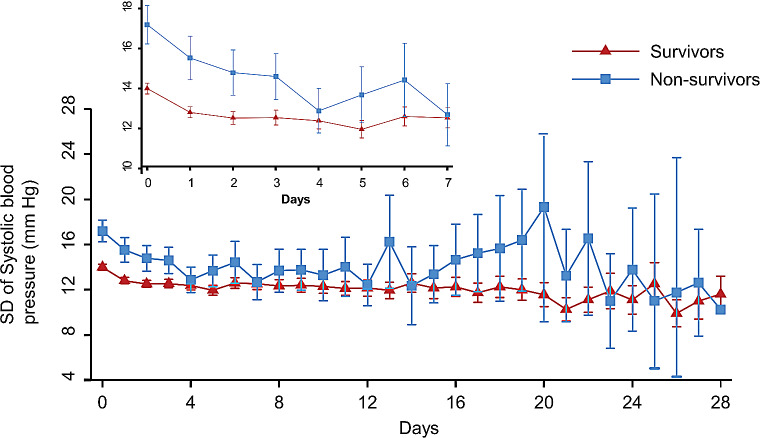
Results: We studied 1486 patients in the hyperacute group and 857 in the acute group. SD of SBP had a significant association with the in-hospital mortality for both the hyperacute group (highest quintile adjusted OR 2.28 95% CI 1.18-4.42; ptrend<0.001) and the acute group (highest quintile adjusted OR 2.17, 95% CI 1.08-4.36; ptrend<0.001). The strongest predictors of primary outcome were SD of SBP in the hyperacute phase and minimum SBP in the acute phase. Associations were similar for the discharge-home rate (for the hyperacute group, highest quintile adjusted OR 0.58, 95% CI 0.37-0.89; ptrend<0.001; for the acute group OR 0.55, 95% CI 0.32-0.95; ptrend<0.001).
Conclusion: Systolic BPV seems to predict a poor outcome in patients with TBI. The benefits of early treatment to maintain appropriate SBP level might be enhanced by smooth and sustained control.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


