{"title":"在内窥镜下插入回肠管,用附着的丝线作为内窥镜的抓取点。","authors":"Yuzo Baba, Masakazu Ueda, Ryo Hashiguchi","doi":"10.1111/den.14900","DOIUrl":null,"url":null,"abstract":"<p>Successful ileus tube (I-tube) insertion requires passing the I-tube into the pylorus,<span><sup>1, 2</sup></span> which may be achieved using an endoscope, and then advancing the I-tube through the duodenum. The latter can be difficult because the force pushing the I-tube may not be effectively transmitted to the tip.<span><sup>3, 4</sup></span> Because the duodenum runs through the retroperitoneum like a tunnel and does not stretch, the I-tube can pass smoothly through the duodenum if directly pushed from inside the stomach, ensuring that the tip does not get trapped into the duodenal folds.</p><p>Here, we propose a new I-tube insertion method that involves attaching grasping points by tying silk threads on the I-tube and pushing the I-tube from inside the stomach with an endoscope (Fig. 1). Specifically, we used a 16F closed-end I-tube with a soft atraumatic tip that was designed to avoid getting trapped into the folds. Silk threads were tied on the I-tube at 5 cm intervals to cover 60 cm from the tip. After the I-tube entered the duodenum, it was pushed by using an endoscope (Fig. 2; Video S1).</p><p>A 60-year-old man underwent surgery for an abdominal aortic aneurysm. The patient presented with abdominal distention and was suspected to have a combination of paralytic ileus and adhesive intestinal obstruction. Endoscopic I-tube insertion was performed on the sixth operative day. Insertion to a depth of 60 cm into the pylorus was smoothly completed within 6 min, with the balloon successfully entering the jejunum. The patient was discharged on the 27th postoperative day.</p><p>The body of the designed I-tube showed sufficient stiffness to not require the use of a guidewire, and the I-tube did not retract during endoscope removal. Insertion was performed in 14 cases and was successful in all cases. The proposed use of an I-tube with endoscope grasping points is a promising method for rapid and simple ileus tube insertion.<span><sup>2, 5</sup></span></p><p>Author Y.B. holds a United States Patent on the naso-jejunal medical tubes (Patent No. US10,524,988 B2). The other authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 11","pages":"1282-1283"},"PeriodicalIF":5.0000,"publicationDate":"2024-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14900","citationCount":"0","resultStr":"{\"title\":\"Endoscopic insertion of an ileus tube with attached silk threads as endoscope grasping points\",\"authors\":\"Yuzo Baba, Masakazu Ueda, Ryo Hashiguchi\",\"doi\":\"10.1111/den.14900\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Successful ileus tube (I-tube) insertion requires passing the I-tube into the pylorus,<span><sup>1, 2</sup></span> which may be achieved using an endoscope, and then advancing the I-tube through the duodenum. The latter can be difficult because the force pushing the I-tube may not be effectively transmitted to the tip.<span><sup>3, 4</sup></span> Because the duodenum runs through the retroperitoneum like a tunnel and does not stretch, the I-tube can pass smoothly through the duodenum if directly pushed from inside the stomach, ensuring that the tip does not get trapped into the duodenal folds.</p><p>Here, we propose a new I-tube insertion method that involves attaching grasping points by tying silk threads on the I-tube and pushing the I-tube from inside the stomach with an endoscope (Fig. 1). Specifically, we used a 16F closed-end I-tube with a soft atraumatic tip that was designed to avoid getting trapped into the folds. Silk threads were tied on the I-tube at 5 cm intervals to cover 60 cm from the tip. After the I-tube entered the duodenum, it was pushed by using an endoscope (Fig. 2; Video S1).</p><p>A 60-year-old man underwent surgery for an abdominal aortic aneurysm. The patient presented with abdominal distention and was suspected to have a combination of paralytic ileus and adhesive intestinal obstruction. Endoscopic I-tube insertion was performed on the sixth operative day. Insertion to a depth of 60 cm into the pylorus was smoothly completed within 6 min, with the balloon successfully entering the jejunum. The patient was discharged on the 27th postoperative day.</p><p>The body of the designed I-tube showed sufficient stiffness to not require the use of a guidewire, and the I-tube did not retract during endoscope removal. Insertion was performed in 14 cases and was successful in all cases. The proposed use of an I-tube with endoscope grasping points is a promising method for rapid and simple ileus tube insertion.<span><sup>2, 5</sup></span></p><p>Author Y.B. holds a United States Patent on the naso-jejunal medical tubes (Patent No. US10,524,988 B2). The other authors declare no conflict of interest for this article.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 11\",\"pages\":\"1282-1283\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-08-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14900\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14900\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14900","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
成功插入回流管(I-tube)需要将 I-tube插入幽门1, 2 ,可以使用内窥镜,然后将 I-tube推进十二指肠。后者可能比较困难,因为推动 I 型管的力量可能无法有效传导到管尖、4 由于十二指肠像隧道一样穿过腹膜后腔,且不伸展,因此如果直接从胃内推动 I 型管,则可以顺利通过十二指肠,确保管尖不会陷入十二指肠皱褶。在此,我们提出了一种新的 I 型管插入方法,即通过在 I 型管上绑丝线来固定抓取点,然后用内窥镜从胃内推动 I 型管(图 1)。具体来说,我们使用的是 16F 的闭端 I 型管,其软性无创伤的顶端设计可避免陷入褶皱。每隔 5 厘米在 I 型管上绑上丝线,覆盖从顶端起 60 厘米的范围。I 型管进入十二指肠后,使用内窥镜将其推入(图 2;视频 S1)。患者出现腹胀,怀疑合并麻痹性回肠炎和粘连性肠梗阻。手术第六天进行了内镜下 I 型管插入术。在 6 分钟内顺利插入幽门 60 厘米深处,球囊成功进入空肠。患者于术后第 27 天出院。所设计的 I 型管管体显示出足够的硬度,无需使用导丝,而且在内窥镜移除过程中,I 型管没有回缩。在 14 个病例中均成功插入了 I 型管。建议使用带有内窥镜抓取点的 I 型管是一种快速、简单插入回肠管的可行方法。其他作者声明与本文无利益冲突。
Endoscopic insertion of an ileus tube with attached silk threads as endoscope grasping points
Successful ileus tube (I-tube) insertion requires passing the I-tube into the pylorus,1, 2 which may be achieved using an endoscope, and then advancing the I-tube through the duodenum. The latter can be difficult because the force pushing the I-tube may not be effectively transmitted to the tip.3, 4 Because the duodenum runs through the retroperitoneum like a tunnel and does not stretch, the I-tube can pass smoothly through the duodenum if directly pushed from inside the stomach, ensuring that the tip does not get trapped into the duodenal folds.
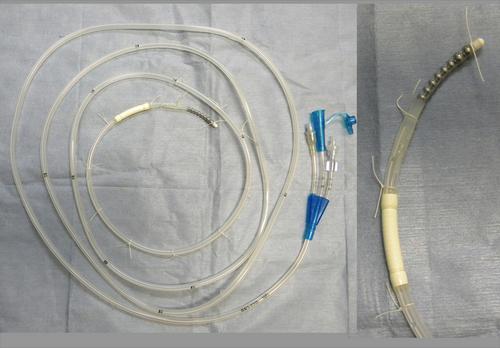
Here, we propose a new I-tube insertion method that involves attaching grasping points by tying silk threads on the I-tube and pushing the I-tube from inside the stomach with an endoscope (Fig. 1). Specifically, we used a 16F closed-end I-tube with a soft atraumatic tip that was designed to avoid getting trapped into the folds. Silk threads were tied on the I-tube at 5 cm intervals to cover 60 cm from the tip. After the I-tube entered the duodenum, it was pushed by using an endoscope (Fig. 2; Video S1).
A 60-year-old man underwent surgery for an abdominal aortic aneurysm. The patient presented with abdominal distention and was suspected to have a combination of paralytic ileus and adhesive intestinal obstruction. Endoscopic I-tube insertion was performed on the sixth operative day. Insertion to a depth of 60 cm into the pylorus was smoothly completed within 6 min, with the balloon successfully entering the jejunum. The patient was discharged on the 27th postoperative day.
The body of the designed I-tube showed sufficient stiffness to not require the use of a guidewire, and the I-tube did not retract during endoscope removal. Insertion was performed in 14 cases and was successful in all cases. The proposed use of an I-tube with endoscope grasping points is a promising method for rapid and simple ileus tube insertion.2, 5
Author Y.B. holds a United States Patent on the naso-jejunal medical tubes (Patent No. US10,524,988 B2). The other authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


