Shalini Nair, Atul More, Reka Karupassamy, Ajith Sivadasan, Sanjith Aaron
{"title":"通过超声波评估膈肌功能来预测神经肌肉疾病患者的机械通气需求及其解放:一项观察性队列试点研究。","authors":"Shalini Nair, Atul More, Reka Karupassamy, Ajith Sivadasan, Sanjith Aaron","doi":"10.1007/s12028-024-02074-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of assisted ventilation and determining the optimal timing for discontinuation presents a significant clinical obstacle in patients affected by neuromuscular (NM) diseases. This study aimed to evaluate the efficacy of ultrasound in appraising diaphragmatic function for predicting the necessity of intubation and determining the opportune moment to discontinue mechanical ventilation (MV) in patients with NM disorders.</p><p><strong>Methods: </strong>The study was conducted in adult patients with NM diseases requiring inpatient care in the high-dependency neurology ward and the intensive care unit. Ultrasonographic assessment of diaphragmatic excursion (DE) and diaphragmatic thickness fraction (DTF) was conducted at the patient's bedside every 48 h for ventilated patients and every 72 h for nonventilated patients until they were weaned from the ventilator or discharged home. Qualitative data are expressed as percentages or numbers, and quantitative data are represented as mean ± standard deviation. Unpaired t-tests were employed to compare continuous variables, and χ<sup>2</sup> tests were used for categorical variables. Contingency table analysis was used to compute relative risks in comparing the baseline DE and DTF with the sequential changes in these values.</p><p><strong>Results: </strong>In cases in which the baseline left DE measured less than 1 cm, the relative risk for the requirement of ventilation was 2.5 times higher, with a confidence interval of 0.62-0.99 (P = 0.19). Notably, a bilateral reduction in DE within the initial 48 h of admission was identified as predictive of need for intubation. When comparing ventilated and nonventilated patients, it was observed that the mean DE values for the left and right sides in ventilated patients (0.74 and 0.79) were significantly lower than those in nonventilated patients (1.3 and 1.66), with corresponding P values of 0.05 and 0.01, respectively. Furthermore, a decline in right DE by more than 50% within 72 h of admission presented a relative risk of 3.3 for the necessity of ventilation, with a confidence interval of 1.29-8.59 (P = 0.01). Duration of ventilation ranged from 2 to 45 days, with an average of 13.14 days, whereas the mean ventilator-free days recorded was 13.57. Notably, a sequential increase in bilateral DE correlated with an extended duration of ventilator-free days.</p><p><strong>Conclusions: </strong>The presence of a baseline left DE of less than 1 cm, a consecutive decrease in DE measurements within 48 h, and a comparative reduction in right DE of more than 50% within the initial 3 days are indicators associated with the requirement for MV in patients with NM disease. Furthermore, the upward trajectory of DE in mechanically ventilated patients is linked to an increased number of days free from ventilator support, suggesting its potential to forecast earlier weaning.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"232-240"},"PeriodicalIF":3.1000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Ultrasonographic Assessment of Diaphragm Function to Predict Need for Mechanical Ventilation and its Liberation in Patients with Neuromuscular Disorders: An Observational Cohort Pilot Study.\",\"authors\":\"Shalini Nair, Atul More, Reka Karupassamy, Ajith Sivadasan, Sanjith Aaron\",\"doi\":\"10.1007/s12028-024-02074-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Management of assisted ventilation and determining the optimal timing for discontinuation presents a significant clinical obstacle in patients affected by neuromuscular (NM) diseases. This study aimed to evaluate the efficacy of ultrasound in appraising diaphragmatic function for predicting the necessity of intubation and determining the opportune moment to discontinue mechanical ventilation (MV) in patients with NM disorders.</p><p><strong>Methods: </strong>The study was conducted in adult patients with NM diseases requiring inpatient care in the high-dependency neurology ward and the intensive care unit. Ultrasonographic assessment of diaphragmatic excursion (DE) and diaphragmatic thickness fraction (DTF) was conducted at the patient's bedside every 48 h for ventilated patients and every 72 h for nonventilated patients until they were weaned from the ventilator or discharged home. Qualitative data are expressed as percentages or numbers, and quantitative data are represented as mean ± standard deviation. Unpaired t-tests were employed to compare continuous variables, and χ<sup>2</sup> tests were used for categorical variables. Contingency table analysis was used to compute relative risks in comparing the baseline DE and DTF with the sequential changes in these values.</p><p><strong>Results: </strong>In cases in which the baseline left DE measured less than 1 cm, the relative risk for the requirement of ventilation was 2.5 times higher, with a confidence interval of 0.62-0.99 (P = 0.19). Notably, a bilateral reduction in DE within the initial 48 h of admission was identified as predictive of need for intubation. When comparing ventilated and nonventilated patients, it was observed that the mean DE values for the left and right sides in ventilated patients (0.74 and 0.79) were significantly lower than those in nonventilated patients (1.3 and 1.66), with corresponding P values of 0.05 and 0.01, respectively. Furthermore, a decline in right DE by more than 50% within 72 h of admission presented a relative risk of 3.3 for the necessity of ventilation, with a confidence interval of 1.29-8.59 (P = 0.01). Duration of ventilation ranged from 2 to 45 days, with an average of 13.14 days, whereas the mean ventilator-free days recorded was 13.57. Notably, a sequential increase in bilateral DE correlated with an extended duration of ventilator-free days.</p><p><strong>Conclusions: </strong>The presence of a baseline left DE of less than 1 cm, a consecutive decrease in DE measurements within 48 h, and a comparative reduction in right DE of more than 50% within the initial 3 days are indicators associated with the requirement for MV in patients with NM disease. Furthermore, the upward trajectory of DE in mechanically ventilated patients is linked to an increased number of days free from ventilator support, suggesting its potential to forecast earlier weaning.</p>\",\"PeriodicalId\":19118,\"journal\":{\"name\":\"Neurocritical Care\",\"volume\":\" \",\"pages\":\"232-240\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurocritical Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12028-024-02074-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-024-02074-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/2 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:对于受神经肌肉(NM)疾病影响的患者而言,辅助通气的管理和确定最佳停用时机是一个重大的临床障碍。本研究旨在评估超声波在评估膈肌功能方面的功效,以预测插管的必要性,并确定 NM 患者停止机械通气(MV)的最佳时机:研究对象为需要在神经内科高危病房和重症监护室接受住院治疗的成年 NM 患者。每隔 48 小时在患者床旁对通气患者的膈肌偏移(DE)和膈肌厚度分数(DTF)进行一次超声波评估,每隔 72 小时对不通气患者的膈肌偏移和膈肌厚度分数进行一次超声波评估,直到他们脱离呼吸机或出院回家。定性数据以百分比或数字表示,定量数据以均数 ± 标准差表示。连续变量的比较采用非配对 t 检验,分类变量的比较采用 χ2 检验。在比较基线 DE 和 DTF 与这些值的连续变化时,采用了或然率表分析来计算相对风险:结果:基线左侧 DE 测量值小于 1 厘米时,需要通气的相对风险高出 2.5 倍,置信区间为 0.62-0.99 (P = 0.19)。值得注意的是,入院最初 48 小时内双侧 DE 的减少可预测是否需要插管。在对通气和不通气患者进行比较时发现,通气患者左侧和右侧的平均 DE 值(0.74 和 0.79)明显低于不通气患者(1.3 和 1.66),相应的 P 值分别为 0.05 和 0.01。此外,入院 72 小时内右侧 DE 下降超过 50%,则需要通气的相对风险为 3.3,置信区间为 1.29-8.59 (P = 0.01)。通气时间从 2 天到 45 天不等,平均为 13.14 天,而无呼吸机记录的平均天数为 13.57 天。值得注意的是,双侧DE的连续增加与无呼吸机天数的延长相关:结论:左侧DE基线小于1厘米、DE测量值在48小时内连续下降、右侧DE在最初3天内相对下降超过50%,这些指标都与NM患者需要使用MV有关。此外,机械通气患者 DE 的上升轨迹与无呼吸机支持天数的增加有关,这表明其有可能预测更早的断气时间。
Ultrasonographic Assessment of Diaphragm Function to Predict Need for Mechanical Ventilation and its Liberation in Patients with Neuromuscular Disorders: An Observational Cohort Pilot Study.
Background: Management of assisted ventilation and determining the optimal timing for discontinuation presents a significant clinical obstacle in patients affected by neuromuscular (NM) diseases. This study aimed to evaluate the efficacy of ultrasound in appraising diaphragmatic function for predicting the necessity of intubation and determining the opportune moment to discontinue mechanical ventilation (MV) in patients with NM disorders.
Methods: The study was conducted in adult patients with NM diseases requiring inpatient care in the high-dependency neurology ward and the intensive care unit. Ultrasonographic assessment of diaphragmatic excursion (DE) and diaphragmatic thickness fraction (DTF) was conducted at the patient's bedside every 48 h for ventilated patients and every 72 h for nonventilated patients until they were weaned from the ventilator or discharged home. Qualitative data are expressed as percentages or numbers, and quantitative data are represented as mean ± standard deviation. Unpaired t-tests were employed to compare continuous variables, and χ2 tests were used for categorical variables. Contingency table analysis was used to compute relative risks in comparing the baseline DE and DTF with the sequential changes in these values.
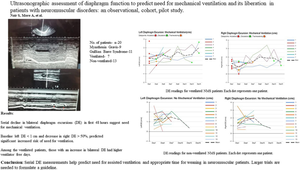
Results: In cases in which the baseline left DE measured less than 1 cm, the relative risk for the requirement of ventilation was 2.5 times higher, with a confidence interval of 0.62-0.99 (P = 0.19). Notably, a bilateral reduction in DE within the initial 48 h of admission was identified as predictive of need for intubation. When comparing ventilated and nonventilated patients, it was observed that the mean DE values for the left and right sides in ventilated patients (0.74 and 0.79) were significantly lower than those in nonventilated patients (1.3 and 1.66), with corresponding P values of 0.05 and 0.01, respectively. Furthermore, a decline in right DE by more than 50% within 72 h of admission presented a relative risk of 3.3 for the necessity of ventilation, with a confidence interval of 1.29-8.59 (P = 0.01). Duration of ventilation ranged from 2 to 45 days, with an average of 13.14 days, whereas the mean ventilator-free days recorded was 13.57. Notably, a sequential increase in bilateral DE correlated with an extended duration of ventilator-free days.
Conclusions: The presence of a baseline left DE of less than 1 cm, a consecutive decrease in DE measurements within 48 h, and a comparative reduction in right DE of more than 50% within the initial 3 days are indicators associated with the requirement for MV in patients with NM disease. Furthermore, the upward trajectory of DE in mechanically ventilated patients is linked to an increased number of days free from ventilator support, suggesting its potential to forecast earlier weaning.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


