{"title":"表皮生长因子受体 L858R 点突变和 MET 第 14 号外显子跳越突变的同步双原发性肺腺癌","authors":"Seijitsu Ando, Shinji Futami, Koji Azuma, Kanako Nishimatsu, Takuma Shirasaka, Seigo Minami","doi":"10.14740/jmc4210","DOIUrl":null,"url":null,"abstract":"<p><p>Various driver mutations and the corresponding molecular-targeted drugs have been detected and developed in non-small cell lung cancer. There were many cases in which surgical specimens had happened to find double primary cancers. However, to our knowledge, our case was the first report of synchronous double primary lung adenocarcinomas harboring epidermal growth factor receptor (<i>EGFR</i>) L858R and mesenchymal-to-epithelial transition (<i>MET</i>) exon 14 skipping mutations. A 75-year-old Japanese woman with chronic heart and renal failures was referred to our department because of a growing nodule in the right upper lung field on chest X-ray films. Chest computed tomography (CT) detected a nodule in the right S<sub>1</sub> and another nodule in the left S<sub>1+2</sub>. Bronchoscopic biopsy diagnosed the right S<sub>1</sub> nodule as moderately differentiated adenocarcinoma. Oncomine Dx Target Test Multi-CDx system of the right S<sub>1</sub> adenocarcinoma detected <i>EGFR</i> L858R mutation. The 18<sup>F</sup>-fluorodeoxyglucose positron emission tomography/CT showed abnormal uptakes both in the right S<sub>1</sub> and the left S<sub>1+2</sub> nodules, and in the bilateral inferior paratracheal lymph nodes. We made a diagnosis of c-stage IIIA (cT<sub>1b</sub>N<sub>2</sub>M<sub>0</sub>) of adenocarcinoma in the right S<sub>1</sub> and suspected another primary lung cancer in the left S<sub>1+2</sub>. Considering her general conditions, comorbidities and wishes, we started osimertinib. The right S<sub>1</sub> cancer achieved partial response (PR), while the left S<sub>1+2</sub> nodule and lymph nodes enlarged. Aspiration cytology from the left supraclavicular lymph node showed adenocarcinoma. The FoundationOne<sup>®</sup> Liquid CDx tumor profiling test detected not only <i>EGFR</i> L858R, but also <i>MET</i> exon 14 skipping mutation. We made a diagnosis of another primary adenocarcinoma from the left S<sub>1+2</sub> nodule (cT<sub>1b</sub>N<sub>3</sub>M<sub>0</sub>, c-stage IIIB) with <i>MET</i> mutation, and changed osimertinib to capmatinib. Although the left S<sub>1+2</sub> cancer achieved and maintained PR by capmatinib, the right S<sub>1</sub> cancer increased, and several new metastases appeared. The subsequent switch from capmatinib to osimertinib could not control cancers. In this case, we tried to switch monotherapies from osimertinib to capmatinib for double primary adenocarcinomas harboring different two driver mutations, according to each cancer progression. The temporal and spatial heterogeneity reinforces the need for primary tissue biopsy if dual primaries are suspected. Temporally distinct liquid biopsies, not standard at present, may be considered.</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"15 8","pages":"153-158"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287901/pdf/","citationCount":"0","resultStr":"{\"title\":\"Synchronous Double Primary Lung Adenocarcinomas With <i>EGFR</i> L858R Point Mutation and <i>MET</i> Exon 14 Skipping Mutation.\",\"authors\":\"Seijitsu Ando, Shinji Futami, Koji Azuma, Kanako Nishimatsu, Takuma Shirasaka, Seigo Minami\",\"doi\":\"10.14740/jmc4210\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Various driver mutations and the corresponding molecular-targeted drugs have been detected and developed in non-small cell lung cancer. There were many cases in which surgical specimens had happened to find double primary cancers. However, to our knowledge, our case was the first report of synchronous double primary lung adenocarcinomas harboring epidermal growth factor receptor (<i>EGFR</i>) L858R and mesenchymal-to-epithelial transition (<i>MET</i>) exon 14 skipping mutations. A 75-year-old Japanese woman with chronic heart and renal failures was referred to our department because of a growing nodule in the right upper lung field on chest X-ray films. Chest computed tomography (CT) detected a nodule in the right S<sub>1</sub> and another nodule in the left S<sub>1+2</sub>. Bronchoscopic biopsy diagnosed the right S<sub>1</sub> nodule as moderately differentiated adenocarcinoma. Oncomine Dx Target Test Multi-CDx system of the right S<sub>1</sub> adenocarcinoma detected <i>EGFR</i> L858R mutation. The 18<sup>F</sup>-fluorodeoxyglucose positron emission tomography/CT showed abnormal uptakes both in the right S<sub>1</sub> and the left S<sub>1+2</sub> nodules, and in the bilateral inferior paratracheal lymph nodes. We made a diagnosis of c-stage IIIA (cT<sub>1b</sub>N<sub>2</sub>M<sub>0</sub>) of adenocarcinoma in the right S<sub>1</sub> and suspected another primary lung cancer in the left S<sub>1+2</sub>. Considering her general conditions, comorbidities and wishes, we started osimertinib. The right S<sub>1</sub> cancer achieved partial response (PR), while the left S<sub>1+2</sub> nodule and lymph nodes enlarged. Aspiration cytology from the left supraclavicular lymph node showed adenocarcinoma. The FoundationOne<sup>®</sup> Liquid CDx tumor profiling test detected not only <i>EGFR</i> L858R, but also <i>MET</i> exon 14 skipping mutation. We made a diagnosis of another primary adenocarcinoma from the left S<sub>1+2</sub> nodule (cT<sub>1b</sub>N<sub>3</sub>M<sub>0</sub>, c-stage IIIB) with <i>MET</i> mutation, and changed osimertinib to capmatinib. Although the left S<sub>1+2</sub> cancer achieved and maintained PR by capmatinib, the right S<sub>1</sub> cancer increased, and several new metastases appeared. The subsequent switch from capmatinib to osimertinib could not control cancers. In this case, we tried to switch monotherapies from osimertinib to capmatinib for double primary adenocarcinomas harboring different two driver mutations, according to each cancer progression. The temporal and spatial heterogeneity reinforces the need for primary tissue biopsy if dual primaries are suspected. Temporally distinct liquid biopsies, not standard at present, may be considered.</p>\",\"PeriodicalId\":101328,\"journal\":{\"name\":\"Journal of medical cases\",\"volume\":\"15 8\",\"pages\":\"153-158\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287901/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of medical cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4210\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/5 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Synchronous Double Primary Lung Adenocarcinomas With EGFR L858R Point Mutation and MET Exon 14 Skipping Mutation.
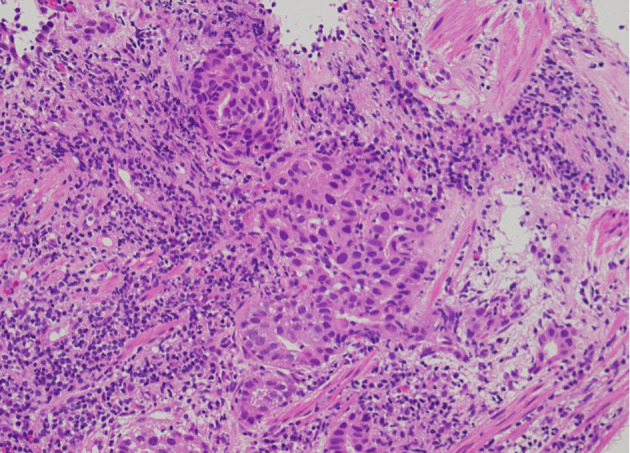
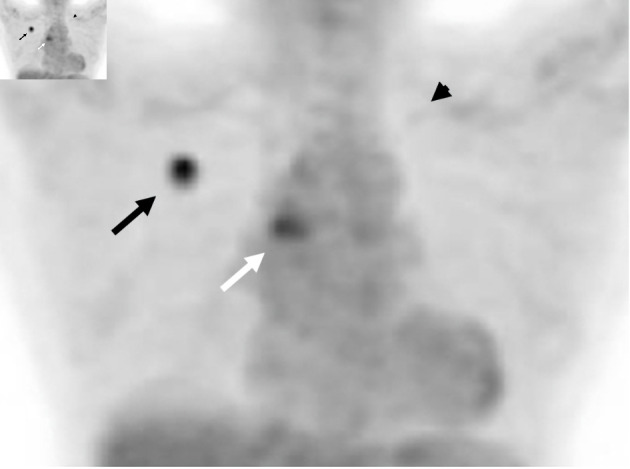
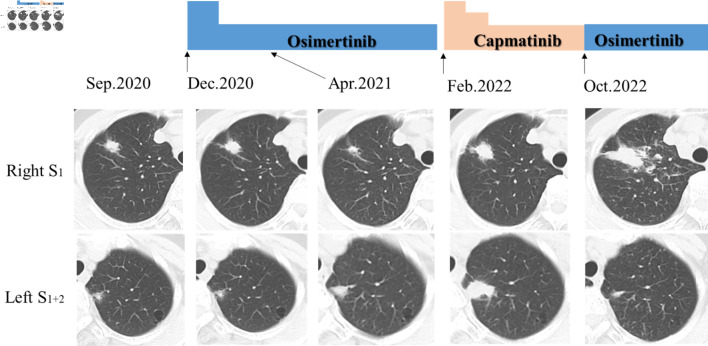
Various driver mutations and the corresponding molecular-targeted drugs have been detected and developed in non-small cell lung cancer. There were many cases in which surgical specimens had happened to find double primary cancers. However, to our knowledge, our case was the first report of synchronous double primary lung adenocarcinomas harboring epidermal growth factor receptor (EGFR) L858R and mesenchymal-to-epithelial transition (MET) exon 14 skipping mutations. A 75-year-old Japanese woman with chronic heart and renal failures was referred to our department because of a growing nodule in the right upper lung field on chest X-ray films. Chest computed tomography (CT) detected a nodule in the right S1 and another nodule in the left S1+2. Bronchoscopic biopsy diagnosed the right S1 nodule as moderately differentiated adenocarcinoma. Oncomine Dx Target Test Multi-CDx system of the right S1 adenocarcinoma detected EGFR L858R mutation. The 18F-fluorodeoxyglucose positron emission tomography/CT showed abnormal uptakes both in the right S1 and the left S1+2 nodules, and in the bilateral inferior paratracheal lymph nodes. We made a diagnosis of c-stage IIIA (cT1bN2M0) of adenocarcinoma in the right S1 and suspected another primary lung cancer in the left S1+2. Considering her general conditions, comorbidities and wishes, we started osimertinib. The right S1 cancer achieved partial response (PR), while the left S1+2 nodule and lymph nodes enlarged. Aspiration cytology from the left supraclavicular lymph node showed adenocarcinoma. The FoundationOne® Liquid CDx tumor profiling test detected not only EGFR L858R, but also MET exon 14 skipping mutation. We made a diagnosis of another primary adenocarcinoma from the left S1+2 nodule (cT1bN3M0, c-stage IIIB) with MET mutation, and changed osimertinib to capmatinib. Although the left S1+2 cancer achieved and maintained PR by capmatinib, the right S1 cancer increased, and several new metastases appeared. The subsequent switch from capmatinib to osimertinib could not control cancers. In this case, we tried to switch monotherapies from osimertinib to capmatinib for double primary adenocarcinomas harboring different two driver mutations, according to each cancer progression. The temporal and spatial heterogeneity reinforces the need for primary tissue biopsy if dual primaries are suspected. Temporally distinct liquid biopsies, not standard at present, may be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


