{"title":"停用 Janus 激酶抑制剂 Ruxolitinib 后的前葡萄膜炎","authors":"Toshihiko Matsuo, Naoto Ikeda, Yasumasa Monobe, Takehiro Tanaka","doi":"10.14740/jmc4274","DOIUrl":null,"url":null,"abstract":"<p><p>Primary myelofibrosis shows widespread fibrosis in the bone marrow and is part of myeloproliferative neoplasms in which gene mutations in hematopoietic stem cells lead to abnormal clonal expansion of one or more lineage of myeloid and erythroid cells and megakaryocytes. Janus kinase (JAK) inhibitors are the main therapeutic regimen for primary myelofibrosis which harbors gene mutations, resulting in continuous activation of JAK-STAT signaling pathway. Since JAK inhibitors modulate immunological state, the administration would have a potential for uveitis. A 67-year-old patient presented with weight loss of 10 kg in the past 2 years after his retirement. He showed normocytic anemia with anisocytosis and abnormal shape, as well as hepatosplenomegaly. Suspected of hematological malignancy, bone marrow biopsy led to the diagnosis of primary myelofibrosis (grade 2) with bizarre megakaryocytes and relative maintenance of myeloid and erythroid lineage. He started to have blood transfusion. Genomic DNA analysis of the peripheral blood showed a pathogenic variant in the exon 9 of calreticulin (<i>CALR</i>) gene while pathogenic variants in Janus kinase-2 (<i>JAK2</i>), and myeloproliferative leukemia virus oncogene (<i>MPL</i>) were absent. He began to have oral ruxolitinib 10 mg daily at the timepoint of 5 months after the initial visit and the dose was increased to 20 mg daily 8 months later but was discontinued further 4 months later because he showed the limited effect of ruxolitinib. He had blood transfusion every week or every 2 weeks in the following 2 months until he noticed blurred vision in the right eye. The right eye showed thick fibrin membrane formation in the anterior chamber in front of the pupil which prevented the fundus from visualization. The left eye showed no inflammation and optic nerve atrophy, sequel to tuberculous meningitis in childhood. The patient started to use 0.1% betamethasone six times daily and 1% atropine once daily as eye drops. A week later, fibrin membrane disappeared and the pupillary area with total iris posterior synechia was visible in the right eye. He regained the vision in the right eye and did not show relapse of uveitis only with topical 0.1% betamethasone. Uveitis might be related with the administration and discontinuation of ruxolitinib.</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"15 8","pages":"208-214"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287903/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anterior Uveitis After Discontinuation of Janus Kinase Inhibitor, Ruxolitinib.\",\"authors\":\"Toshihiko Matsuo, Naoto Ikeda, Yasumasa Monobe, Takehiro Tanaka\",\"doi\":\"10.14740/jmc4274\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Primary myelofibrosis shows widespread fibrosis in the bone marrow and is part of myeloproliferative neoplasms in which gene mutations in hematopoietic stem cells lead to abnormal clonal expansion of one or more lineage of myeloid and erythroid cells and megakaryocytes. Janus kinase (JAK) inhibitors are the main therapeutic regimen for primary myelofibrosis which harbors gene mutations, resulting in continuous activation of JAK-STAT signaling pathway. Since JAK inhibitors modulate immunological state, the administration would have a potential for uveitis. A 67-year-old patient presented with weight loss of 10 kg in the past 2 years after his retirement. He showed normocytic anemia with anisocytosis and abnormal shape, as well as hepatosplenomegaly. Suspected of hematological malignancy, bone marrow biopsy led to the diagnosis of primary myelofibrosis (grade 2) with bizarre megakaryocytes and relative maintenance of myeloid and erythroid lineage. He started to have blood transfusion. Genomic DNA analysis of the peripheral blood showed a pathogenic variant in the exon 9 of calreticulin (<i>CALR</i>) gene while pathogenic variants in Janus kinase-2 (<i>JAK2</i>), and myeloproliferative leukemia virus oncogene (<i>MPL</i>) were absent. He began to have oral ruxolitinib 10 mg daily at the timepoint of 5 months after the initial visit and the dose was increased to 20 mg daily 8 months later but was discontinued further 4 months later because he showed the limited effect of ruxolitinib. He had blood transfusion every week or every 2 weeks in the following 2 months until he noticed blurred vision in the right eye. The right eye showed thick fibrin membrane formation in the anterior chamber in front of the pupil which prevented the fundus from visualization. The left eye showed no inflammation and optic nerve atrophy, sequel to tuberculous meningitis in childhood. The patient started to use 0.1% betamethasone six times daily and 1% atropine once daily as eye drops. A week later, fibrin membrane disappeared and the pupillary area with total iris posterior synechia was visible in the right eye. He regained the vision in the right eye and did not show relapse of uveitis only with topical 0.1% betamethasone. Uveitis might be related with the administration and discontinuation of ruxolitinib.</p>\",\"PeriodicalId\":101328,\"journal\":{\"name\":\"Journal of medical cases\",\"volume\":\"15 8\",\"pages\":\"208-214\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287903/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of medical cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4274\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4274","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Anterior Uveitis After Discontinuation of Janus Kinase Inhibitor, Ruxolitinib.
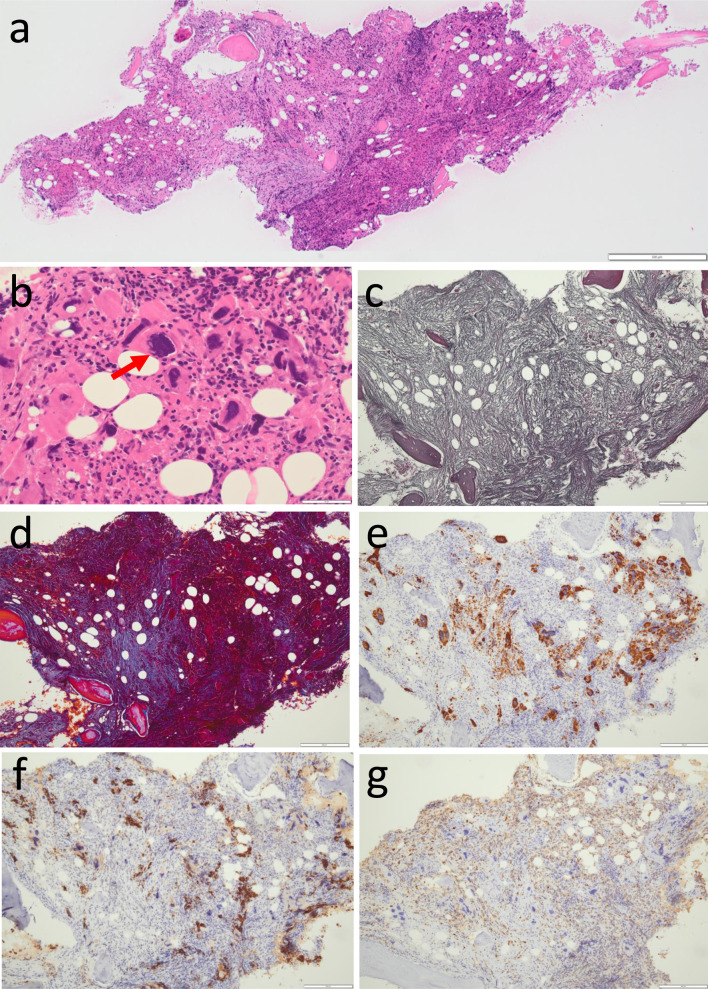
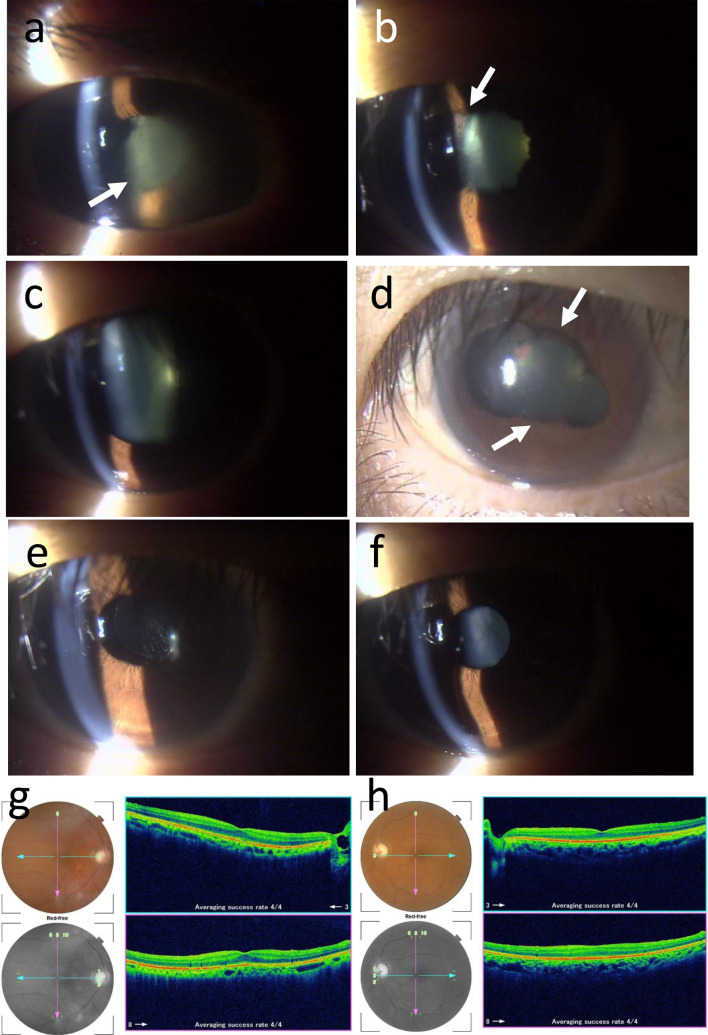
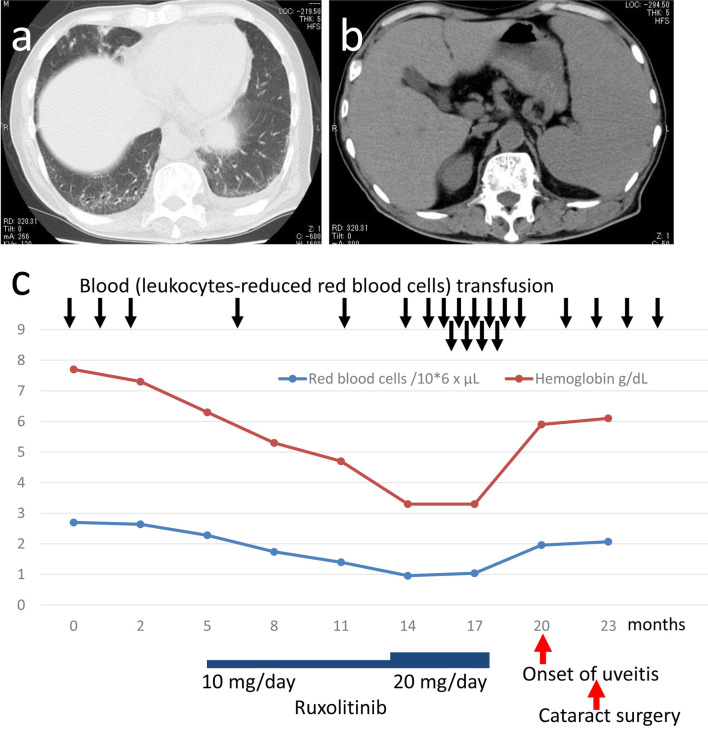
Primary myelofibrosis shows widespread fibrosis in the bone marrow and is part of myeloproliferative neoplasms in which gene mutations in hematopoietic stem cells lead to abnormal clonal expansion of one or more lineage of myeloid and erythroid cells and megakaryocytes. Janus kinase (JAK) inhibitors are the main therapeutic regimen for primary myelofibrosis which harbors gene mutations, resulting in continuous activation of JAK-STAT signaling pathway. Since JAK inhibitors modulate immunological state, the administration would have a potential for uveitis. A 67-year-old patient presented with weight loss of 10 kg in the past 2 years after his retirement. He showed normocytic anemia with anisocytosis and abnormal shape, as well as hepatosplenomegaly. Suspected of hematological malignancy, bone marrow biopsy led to the diagnosis of primary myelofibrosis (grade 2) with bizarre megakaryocytes and relative maintenance of myeloid and erythroid lineage. He started to have blood transfusion. Genomic DNA analysis of the peripheral blood showed a pathogenic variant in the exon 9 of calreticulin (CALR) gene while pathogenic variants in Janus kinase-2 (JAK2), and myeloproliferative leukemia virus oncogene (MPL) were absent. He began to have oral ruxolitinib 10 mg daily at the timepoint of 5 months after the initial visit and the dose was increased to 20 mg daily 8 months later but was discontinued further 4 months later because he showed the limited effect of ruxolitinib. He had blood transfusion every week or every 2 weeks in the following 2 months until he noticed blurred vision in the right eye. The right eye showed thick fibrin membrane formation in the anterior chamber in front of the pupil which prevented the fundus from visualization. The left eye showed no inflammation and optic nerve atrophy, sequel to tuberculous meningitis in childhood. The patient started to use 0.1% betamethasone six times daily and 1% atropine once daily as eye drops. A week later, fibrin membrane disappeared and the pupillary area with total iris posterior synechia was visible in the right eye. He regained the vision in the right eye and did not show relapse of uveitis only with topical 0.1% betamethasone. Uveitis might be related with the administration and discontinuation of ruxolitinib.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


