Alicia Rosenzveig, Amer Jarrar, Tommy Stuleanu, Joseph Mamazza, Amy Neville, Caolan Walsh, Patrick B Murphy, Nicole Kolozsvari
{"title":"加拿大急诊外科学术模式介绍。","authors":"Alicia Rosenzveig, Amer Jarrar, Tommy Stuleanu, Joseph Mamazza, Amy Neville, Caolan Walsh, Patrick B Murphy, Nicole Kolozsvari","doi":"10.1503/cjs.000724","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients who require emergency general surgery (EGS) are at a substantially higher risk for perioperative morbidity and mortality than patients undergoing elective general surgery. The acute care surgery (ACS) model has been shown to improve EGS patient outcomes and cost-effectiveness. A recent systematic review has shown extensive heterogeneity in the structure of ACS models worldwide. The objective of this study was to describe the current landscape of ACS models in academic centres across Canada.</p><p><strong>Methods: </strong>We sent an online questionnaire to the 18 academic centres in Canada. The lead ACS physicians from each institution completed the questionnaire, describing the structure of their ACS models.</p><p><strong>Results: </strong>In total, 16 institutions responded, all of which reported having ACS models, with a total of 29 ACS services described. All services had resident coverage. Of the 29, 18 (62%) had dedicated allied health care staff. The staff surgeon was free from elective duties while covering ACS in 17/29 (59%) services. More than half (15/29; 52%) of the services described protected ACS operating room time, but only 7/15 (47%) had a dedicated ACS room all 5 weekdays. Four of 29 services (14%) had no protected ACS operating room time. Only 1/16 (6%) institutions reported a mandate to conduct ACS research, while 12/16 (75%) found ACS research difficult, owing to lack of resources.</p><p><strong>Conclusion: </strong>We saw large variations in the structure of ACS models in academic centres in Canada. The components of ACS models that are most important to patient outcomes remain poorly defined. Future research will focus on defining the necessary cornerstones of ACS models.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"67 4","pages":"E307-E312"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11300033/pdf/","citationCount":"0","resultStr":"{\"title\":\"A lay of the land: a description of academic acute care surgery models in Canada.\",\"authors\":\"Alicia Rosenzveig, Amer Jarrar, Tommy Stuleanu, Joseph Mamazza, Amy Neville, Caolan Walsh, Patrick B Murphy, Nicole Kolozsvari\",\"doi\":\"10.1503/cjs.000724\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients who require emergency general surgery (EGS) are at a substantially higher risk for perioperative morbidity and mortality than patients undergoing elective general surgery. The acute care surgery (ACS) model has been shown to improve EGS patient outcomes and cost-effectiveness. A recent systematic review has shown extensive heterogeneity in the structure of ACS models worldwide. The objective of this study was to describe the current landscape of ACS models in academic centres across Canada.</p><p><strong>Methods: </strong>We sent an online questionnaire to the 18 academic centres in Canada. The lead ACS physicians from each institution completed the questionnaire, describing the structure of their ACS models.</p><p><strong>Results: </strong>In total, 16 institutions responded, all of which reported having ACS models, with a total of 29 ACS services described. All services had resident coverage. Of the 29, 18 (62%) had dedicated allied health care staff. The staff surgeon was free from elective duties while covering ACS in 17/29 (59%) services. More than half (15/29; 52%) of the services described protected ACS operating room time, but only 7/15 (47%) had a dedicated ACS room all 5 weekdays. Four of 29 services (14%) had no protected ACS operating room time. Only 1/16 (6%) institutions reported a mandate to conduct ACS research, while 12/16 (75%) found ACS research difficult, owing to lack of resources.</p><p><strong>Conclusion: </strong>We saw large variations in the structure of ACS models in academic centres in Canada. The components of ACS models that are most important to patient outcomes remain poorly defined. Future research will focus on defining the necessary cornerstones of ACS models.</p>\",\"PeriodicalId\":9573,\"journal\":{\"name\":\"Canadian Journal of Surgery\",\"volume\":\"67 4\",\"pages\":\"E307-E312\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11300033/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1503/cjs.000724\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.000724","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
A lay of the land: a description of academic acute care surgery models in Canada.
Background: Patients who require emergency general surgery (EGS) are at a substantially higher risk for perioperative morbidity and mortality than patients undergoing elective general surgery. The acute care surgery (ACS) model has been shown to improve EGS patient outcomes and cost-effectiveness. A recent systematic review has shown extensive heterogeneity in the structure of ACS models worldwide. The objective of this study was to describe the current landscape of ACS models in academic centres across Canada.
Methods: We sent an online questionnaire to the 18 academic centres in Canada. The lead ACS physicians from each institution completed the questionnaire, describing the structure of their ACS models.
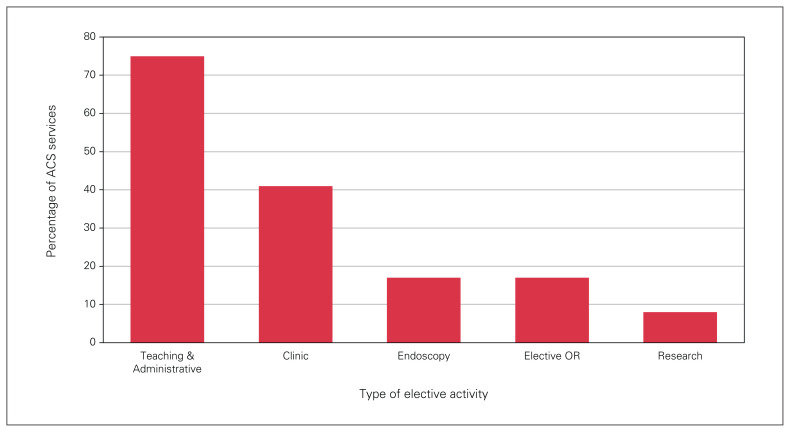
Results: In total, 16 institutions responded, all of which reported having ACS models, with a total of 29 ACS services described. All services had resident coverage. Of the 29, 18 (62%) had dedicated allied health care staff. The staff surgeon was free from elective duties while covering ACS in 17/29 (59%) services. More than half (15/29; 52%) of the services described protected ACS operating room time, but only 7/15 (47%) had a dedicated ACS room all 5 weekdays. Four of 29 services (14%) had no protected ACS operating room time. Only 1/16 (6%) institutions reported a mandate to conduct ACS research, while 12/16 (75%) found ACS research difficult, owing to lack of resources.
Conclusion: We saw large variations in the structure of ACS models in academic centres in Canada. The components of ACS models that are most important to patient outcomes remain poorly defined. Future research will focus on defining the necessary cornerstones of ACS models.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


