{"title":"机器人辅助对比腹腔镜手术在直肠癌侧淋巴结清扫中的疗效和安全性的荟萃分析","authors":"Hao Shi, Xianhao Yi, Xin Yan, Wenjie Wu, Hui Ouyang, Chengke Ou, Xiangheng Chen","doi":"10.1007/s00464-024-11111-3","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>A meta-analysis was conducted on the perioperative and oncological outcomes of robot-assisted and laparoscopic lateral lymph node dissection in rectal cancer. There are few articles and reports on this topic, and a lack of high-quality research results in unreliable research conclusions. This study includes prospective and retrospective studies to obtain more reliable findings.</p><h3 data-test=\"abstract-sub-heading\">Materials and methods</h3><p>Databases were searched, including PubMed, EMBASE, Cochrane, and Web of Science. The search was conducted from the time of database construction to March 2024. The quality of the literature was evaluated using the NOS scoring system. Meta-analysis was performed using R language software. Statistical heterogeneity was assessed using the <i>I</i><sup>2</sup> statistic, and sensitivity analysis was performed.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Six relevant literatures that met the criteria were finally included, and 652 patients were included, including 316 (48.5%) in the robot-assisted lateral lymph node dissection for rectal cancer group (RLLND) and 336 (51.5%) in the laparoscopic lateral lymph node dissection for rectal cancer group (LLLND). Analysis of the results showed that compared with the laparoscopic group, the robotic group had less mean intraoperative blood loss (MD = − 22, 95% CI − 40.03 to − 3.97, <i>P</i> < 0.05), longer operative time (MD = 51.57, 95%CI 7.69 to 95.45, <i>P</i> < 0.05), and a shorter mean hospital stay (MD = − 1.25, 95%CI − 2.46 to − 0.05, <i>P</i> < 0.05), a low rate of urinary complications (OR 0.39, 95%CI 0.23 to 0.64, <i>P</i> < 0.01), a low overall rate of postoperative complications (OR 0.6, 95%CI 0.42 to 0.87, <i>P</i> < 0.01), and a high number of lateral lymph node dissection (MD = 1.18, 95% CI 0.14 to 2.23, <i>P</i> < 0.05), and there was no statistically significant difference between the two groups in terms of postoperative anastomotic leakage, postoperative intestinal obstruction, and total number of lymph nodes obtained (<i>P</i> > 0.05).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Compared with laparoscopy, robotic lateral lymph node dissection for rectal cancer reduces intraoperative blood loss, shortens the average length of hospital stay, reduces urologic complications, decreases overall postoperative complications, and collects more lateral lymph nodes. However, the surgical time is prolonged.</p><h3 data-test=\"abstract-sub-heading\">Graphical abstract</h3>\n","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"109 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Meta-analysis of the efficacy and safety of robot-assisted comparative laparoscopic surgery in lateral lymph node dissection for rectal cancer\",\"authors\":\"Hao Shi, Xianhao Yi, Xin Yan, Wenjie Wu, Hui Ouyang, Chengke Ou, Xiangheng Chen\",\"doi\":\"10.1007/s00464-024-11111-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Introduction</h3><p>A meta-analysis was conducted on the perioperative and oncological outcomes of robot-assisted and laparoscopic lateral lymph node dissection in rectal cancer. There are few articles and reports on this topic, and a lack of high-quality research results in unreliable research conclusions. This study includes prospective and retrospective studies to obtain more reliable findings.</p><h3 data-test=\\\"abstract-sub-heading\\\">Materials and methods</h3><p>Databases were searched, including PubMed, EMBASE, Cochrane, and Web of Science. The search was conducted from the time of database construction to March 2024. The quality of the literature was evaluated using the NOS scoring system. Meta-analysis was performed using R language software. Statistical heterogeneity was assessed using the <i>I</i><sup>2</sup> statistic, and sensitivity analysis was performed.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>Six relevant literatures that met the criteria were finally included, and 652 patients were included, including 316 (48.5%) in the robot-assisted lateral lymph node dissection for rectal cancer group (RLLND) and 336 (51.5%) in the laparoscopic lateral lymph node dissection for rectal cancer group (LLLND). Analysis of the results showed that compared with the laparoscopic group, the robotic group had less mean intraoperative blood loss (MD = − 22, 95% CI − 40.03 to − 3.97, <i>P</i> < 0.05), longer operative time (MD = 51.57, 95%CI 7.69 to 95.45, <i>P</i> < 0.05), and a shorter mean hospital stay (MD = − 1.25, 95%CI − 2.46 to − 0.05, <i>P</i> < 0.05), a low rate of urinary complications (OR 0.39, 95%CI 0.23 to 0.64, <i>P</i> < 0.01), a low overall rate of postoperative complications (OR 0.6, 95%CI 0.42 to 0.87, <i>P</i> < 0.01), and a high number of lateral lymph node dissection (MD = 1.18, 95% CI 0.14 to 2.23, <i>P</i> < 0.05), and there was no statistically significant difference between the two groups in terms of postoperative anastomotic leakage, postoperative intestinal obstruction, and total number of lymph nodes obtained (<i>P</i> > 0.05).</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>Compared with laparoscopy, robotic lateral lymph node dissection for rectal cancer reduces intraoperative blood loss, shortens the average length of hospital stay, reduces urologic complications, decreases overall postoperative complications, and collects more lateral lymph nodes. However, the surgical time is prolonged.</p><h3 data-test=\\\"abstract-sub-heading\\\">Graphical abstract</h3>\\n\",\"PeriodicalId\":501625,\"journal\":{\"name\":\"Surgical Endoscopy\",\"volume\":\"109 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Endoscopy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s00464-024-11111-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-11111-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
引言 一项荟萃分析针对直肠癌机器人辅助和腹腔镜侧淋巴结清扫术的围手术期和肿瘤学结果进行了研究。有关这一主题的文章和报告很少,缺乏高质量的研究导致研究结论不可靠。本研究包括前瞻性研究和回顾性研究,以获得更可靠的结论。材料和方法检索数据库,包括PubMed、EMBASE、Cochrane和Web of Science。检索时间为数据库建立后至 2024 年 3 月。文献质量采用 NOS 评分系统进行评估。使用 R 语言软件进行元分析。结果最终纳入了6篇符合标准的相关文献,共纳入652例患者,其中机器人辅助直肠癌侧淋巴结清扫术(RLLND)组316例(48.5%),腹腔镜直肠癌侧淋巴结清扫术(LLLND)组336例(51.5%)。结果分析表明,与腹腔镜组相比,机器人组术中平均失血量更少(MD = - 22,95%CI - 40.03 to - 3.97,P < 0.05),手术时间更长(MD = 51.57,95%CI 7.69 to 95.45,P < 0.05),平均住院时间更短(MD = - 1.25,95%CI - 2.46 to - 0.05,P < 0.05),泌尿系统并发症发生率低(OR 0.39,95%CI 0.23 to 0.64,P < 0.01),术后并发症总发生率低(OR 0.6,95%CI 0.42 to 0.87,P < 0.01),侧淋巴结清扫次数多(MD = 1.18, 95% CI 0.14 to 2.23, P <0.05),两组在术后吻合口漏、术后肠梗阻、获得淋巴结总数方面差异无统计学意义(P >0.05)。结论与腹腔镜相比,机器人侧淋巴结清扫术治疗直肠癌减少了术中失血,缩短了平均住院时间,减少了泌尿系统并发症,降低了整体术后并发症,并收集了更多的侧淋巴结。但手术时间延长。
Meta-analysis of the efficacy and safety of robot-assisted comparative laparoscopic surgery in lateral lymph node dissection for rectal cancer
Introduction
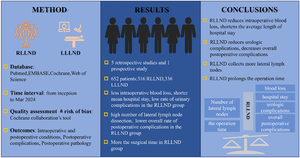
A meta-analysis was conducted on the perioperative and oncological outcomes of robot-assisted and laparoscopic lateral lymph node dissection in rectal cancer. There are few articles and reports on this topic, and a lack of high-quality research results in unreliable research conclusions. This study includes prospective and retrospective studies to obtain more reliable findings.
Materials and methods
Databases were searched, including PubMed, EMBASE, Cochrane, and Web of Science. The search was conducted from the time of database construction to March 2024. The quality of the literature was evaluated using the NOS scoring system. Meta-analysis was performed using R language software. Statistical heterogeneity was assessed using the I2 statistic, and sensitivity analysis was performed.
Results
Six relevant literatures that met the criteria were finally included, and 652 patients were included, including 316 (48.5%) in the robot-assisted lateral lymph node dissection for rectal cancer group (RLLND) and 336 (51.5%) in the laparoscopic lateral lymph node dissection for rectal cancer group (LLLND). Analysis of the results showed that compared with the laparoscopic group, the robotic group had less mean intraoperative blood loss (MD = − 22, 95% CI − 40.03 to − 3.97, P < 0.05), longer operative time (MD = 51.57, 95%CI 7.69 to 95.45, P < 0.05), and a shorter mean hospital stay (MD = − 1.25, 95%CI − 2.46 to − 0.05, P < 0.05), a low rate of urinary complications (OR 0.39, 95%CI 0.23 to 0.64, P < 0.01), a low overall rate of postoperative complications (OR 0.6, 95%CI 0.42 to 0.87, P < 0.01), and a high number of lateral lymph node dissection (MD = 1.18, 95% CI 0.14 to 2.23, P < 0.05), and there was no statistically significant difference between the two groups in terms of postoperative anastomotic leakage, postoperative intestinal obstruction, and total number of lymph nodes obtained (P > 0.05).
Conclusion
Compared with laparoscopy, robotic lateral lymph node dissection for rectal cancer reduces intraoperative blood loss, shortens the average length of hospital stay, reduces urologic complications, decreases overall postoperative complications, and collects more lateral lymph nodes. However, the surgical time is prolonged.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


