Iris K. Minichmayr, Tomoyuki Mizuno, Srijib Goswami, Richard W. Peck, Thomas M. Polasek, the American Society of Clinical Pharmacology and Therapeutics Precision Dosing Community
{"title":"应对精准给药挑战的最新进展。","authors":"Iris K. Minichmayr, Tomoyuki Mizuno, Srijib Goswami, Richard W. Peck, Thomas M. Polasek, the American Society of Clinical Pharmacology and Therapeutics Precision Dosing Community","doi":"10.1002/cpt.3365","DOIUrl":null,"url":null,"abstract":"<p>Precision dosing can improve drug therapy in complex, critically ill, and chronically ill patient populations who exhibit vast interindividual variabilities in exposures and responses. This perspective outlines five major challenges in precision dosing and highlights their recent progress: (1) application in drug development, (2) improved clinical trials, (3) usefulness of response biomarkers, (4) confidence in model-informed precision dosing, and (5) receptiveness in clinical practice. Many outstanding opportunities in precision dosing remain within regulatory frameworks, data integration and protection, ethics, and reimbursement strategies.</p><p>Precision dosing is a foundational pillar of personalized medicine. The term has been applied to different dosing strategies aimed at improving outcomes and safety in complex patients displaying substantial interindividual variability in drug exposure and response. Depending on their degree of individualization, various “precision dosing methods” result in dosing recommendations for patient subgroups based on specific indications, genotypes, or patient characteristics like renal function, and/or in more individualized dosing based on measurements obtained during drug treatment, for example, drug concentrations from therapeutic drug monitoring (TDM). In complex situations in which target effect measurement and data interpretation are not straightforward, multiple pieces rather than a single pieces of information are ideally combined for precision dosing, requiring sophisticated predictive models.</p><p>Over the past 5–10 years, precision dosing activities, ranging from dried blood spot analyses of plasma drug concentrations to novel models and educational initiatives fostering better collaboration, have surged, with the goals of benefiting patients, aiding prescribers, saving money, and supporting the development of difficult-to-use drugs. This perspective describes recent advances that address five major challenges of precision dosing (<b>Figure</b> 1), followed by a summary of other challenges with slow progress.</p><p>There are strong economic and logistical reasons to limit the number of test doses studied in clinical development. Despite these challenges, precision dosing may be invaluable in tackling complex drug development scenarios, such as for (1) drugs with narrow therapeutic windows, (2) drugs that can lead to severe adverse effects at otherwise typical doses, (3) drugs used for conditions like cancer that carry serious consequences if undertreated, (4) drugs for treating rare, severe, and progressive diseases, and (5) drugs requiring invasive administration routes, for example, intravitreal or intrathecal.<span><sup>1</sup></span></p><p>Regulatory support is variable, but a successful example of pharma-regulatory collaboration supporting precision dosing is MyPKFit®, a clinical decision support (CDS) tool approved alongside recombinant factor VIII that personalizes dosing in hemophilia A. Also, the ophthalmologic drug faricimab was developed with a precision dosing arm in all four of its pivotal clinical trials, covering two indications, that is, neovascular age-related macular degeneration and diabetic macular edema. Personalized treatment with faricimab was approved, with dosing interval individualization according to disease activity such as visual outcomes.<span><sup>1</sup></span></p><p>Generating clinical trial evidence for precision dosing poses a significant challenge with much progress in recent years. As confidence in dose predictions increases (Challenge 4), incorporating MIPD into prospective clinical trials, such as concentration-controlled or effect-controlled trials, is becoming more common.</p><p>Phase II and III studies with individualized dosing arms rather than fixed dosing arms facilitate the exploration of wider and more nuanced doses, resulting in the approval of dose ranges, and subsequently reduced necessity for off-label dosing. Clinical trials of GLP-1 agonists use this approach because there is a fine balance between efficacy and gastrointestinal intolerance.<span><sup>2</sup></span></p><p>In 2021, the FDA's Oncology Center of Excellence initiated Project Optimus to reform the dose selection paradigm in oncology drug development. Project Optimus's primary goal is to ensure that new cancer drugs are developed with optimal dosing strategies by leveraging modern clinical trial designs and more adaptable, patient-centered approaches to dosing – instead of the conventional maximum tolerated dose approach – that consider individual variability and the unique characteristics of the respective cancer type.</p><p>Substantial portions of pharmacokinetic-pharmacodynamic (PK-PD) variability remain unknown for many drugs. Efforts to further understand disease heterogeneity and variability in drug responses, even among patients with comparable drug exposures, have significantly increased in the last decade with the discovery of novel biomarkers and the development of new, more sensitive analysis methods.</p><p>For certain drugs, TDM utilizing microsampling devices – allowing dried blood spot collection at home and delivery to a laboratory for concentration testing – is feasible.<span><sup>3</sup></span> Furthermore, recent advances in biosensor technology have improved the ability to measure drug concentrations directly and non-invasively.<span><sup>4</sup></span> This extends to biomarker monitoring, exemplified by the boom in continuous blood glucose monitoring patches that provide feedback on antidiabetic drug responses.</p><p>Wearable devices further allow noninvasive and real-time collection of various vital signs and health-related data, including heart rate, blood pressure, and other biomarkers. Considering these data in MIPD systems holds promise for precision dosing, not only relying on PK parameters (e.g., trough concentrations or area under the plasma drug concentration-time curve results, AUC), but also leveraging novel PD biomarkers and clinical- or patient-related treatment outcomes. Quantitative systems pharmacology and disease modeling can provide a mechanistic framework to integrate PD biomarkers that predict disease progression, treatment response, and drug safety.<span><sup>5</sup></span></p><p>Finally, with the improved ability to collect and securely store extensive amounts of data from both clinical trial and real-world settings, artificial intelligence and machine learning (AI-ML) are growing in importance for identifying patterns of covariates associated with certain clinical outcomes, which could ultimately inform optimal dosing strategies for individual patients.<span><sup>1</sup></span></p><p>Recent technological advancements and research efforts have significantly improved the feasibility of precision dosing in highly complex patients. Evolving MIPD approaches now offer a framework to simultaneously integrate several patient-, drug-, and disease-related covariates known to influence drug exposures and responses.</p><p>A MIPD approach with proof-of-concept data that is yet to be applied prospectively in the clinic is physiologically-based pharmacokinetic (PBPK) modeling and simulation. The terms “virtual twins” and “digital twins” have been coined to describe this type of MIPD, which simulates an individual's PK profile based on their physiology and health status. It is especially appealing for drugs with established target exposure ranges and for special, understudied populations of patients (e.g., children, pregnant women, and lactating mothers) in whom dosing recommendations are unavailable, or when population PK models to guide dosing do not exist.</p><p>AI-ML methods are increasingly studied in precision dosing to predict drug exposure, the incidence of adverse drug reactions, efficacy, or other outcomes.<span><sup>6</sup></span> Examples of pioneering work include the utilization of extreme gradient boosting (XGBoost) models to predict exposures to tacrolimus and mycophenolic acid in support of precision dosing of immunosuppressants.<span><sup>7</sup></span> Additionally, hybrid ML-PK-PD methods, merging AI-ML with traditional pharmacometric approaches, have been investigated to support MIPD systems. A recent study demonstrated that simulation-based data augmentation and enrichment of ML model features with PK-PD model predictions enhanced the predictive ability of the ML model in forecasting chemotherapy-induced neutropenia.<span><sup>8</sup></span> Continuous learning and other approaches to refine PK-PD model parameters and continuously update models used for MIPD have been proposed, and AI-ML could facilitate these processes automatically or semi-automatically as new clinical data are collected through electronic health records (EHRs). In addition, reinforcement learning constitutes a promising approach to enhancing MIPD with the capability of continuous learning.</p><p>Complex dosing and monitoring are difficult to implement, and more advanced precision dosing approaches, including pharmacogenomic (PGx)-guided dosing, are often limited to a few specialties, e.g. hematology, oncology, or pediatrics.<span><sup>9</sup></span> To address clinical implementation, major steps forward in developing user-friendly precision dosing solutions have been achieved in recent years. Furthermore, the successful establishment of precision dosing CDS tools encompasses strategic planning, seamless integration into existing workflows, and continuous improvement. Coupled with the adoption of FHIR (Fast Healthcare Interoperability Resources) standards, these systems can be integrated with major EHRs, paving the way for broader adoption. Companies such as InsightRx and DoseMeRx have successfully demonstrated these integration capabilities for MIPD of approved drugs requiring TDM, including various antimicrobials, immunosuppressants, and anticancer drugs. Moreover, the scope of data within EHRs has been broadening to include a variety of relevant biomarkers and genetic information, facilitating PGx-guided dosing.</p><p>Professional societies are increasingly taking the lead on precision dosing guidelines. This sets the precedent that adherence to drug labeling is softened by professional consensus. Vancomycin dosing and TDM guidelines in 2020 marked a significant milestone in this regard, catalyzing several health systems to implement MIPD strategies aimed at achieving targeted AUC metrics.<span><sup>10</sup></span></p><p>Diverse types of information can inform precision dosing, though necessitating efficient and safe integration from different data sources. The importance of data sharing, while adhering to data protection and privacy regulations, and sometimes with competing commercial interests (e.g., pathology providers), is not to be underestimated, and must be solved for more complex precision dosing approaches to succeed.</p><p>Once precision dosing has been implemented in practice, clinical trials and real-world evidence investigating its benefits over standard approaches are crucial to increase acceptance and foster more widespread adoption. Challenges of conducting such studies include the selection of appropriate precision dosing targets, appropriate end points (e.g., clinical- and patient-reported outcomes), and timing.</p><p>Precision dosing requires additional ethical and legal considerations, including consent from patients and legal protection for prescribers when doses different from those approved are used in the spirit of beneficence. This would be facilitated when guidelines are available from professional societies (Challenge 5).</p><p>Finally, novel reimbursement models for drug therapies are required to encourage precision dosing in drug development and clinical practice. For example, therapy prices independent of the prescribed dose, including outcome-based reimbursement, would accelerate the adoption of precision dosing.</p><p>This perspective emphasizes recent advances in precision dosing and outlines some outstanding opportunities. As precision dosing evolves, greater integration into drug development and clinical practice holds promise to significantly advance personalized medicine, offering more tailored, effective, and safe drug treatments for more patients.</p><p>No funding was received for this work.</p><p>IKM, TM, and TMP declare no conflicts of interest. RWP holds stock in and receives compensation from F Hoffmann la Roche. SG is employed by InsightRx, which produces model-informed precision dosing clinical decision support tools. As an Associate Editor for Clinical Pharmacology & Therapeutics, Iris Minichmayr was not involved in the review or decision process for this paper.</p>","PeriodicalId":153,"journal":{"name":"Clinical Pharmacology & Therapeutics","volume":null,"pages":null},"PeriodicalIF":6.3000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3365","citationCount":"0","resultStr":"{\"title\":\"Recent Advances Addressing the Challenges of Precision Dosing\",\"authors\":\"Iris K. Minichmayr, Tomoyuki Mizuno, Srijib Goswami, Richard W. Peck, Thomas M. Polasek, the American Society of Clinical Pharmacology and Therapeutics Precision Dosing Community\",\"doi\":\"10.1002/cpt.3365\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Precision dosing can improve drug therapy in complex, critically ill, and chronically ill patient populations who exhibit vast interindividual variabilities in exposures and responses. This perspective outlines five major challenges in precision dosing and highlights their recent progress: (1) application in drug development, (2) improved clinical trials, (3) usefulness of response biomarkers, (4) confidence in model-informed precision dosing, and (5) receptiveness in clinical practice. Many outstanding opportunities in precision dosing remain within regulatory frameworks, data integration and protection, ethics, and reimbursement strategies.</p><p>Precision dosing is a foundational pillar of personalized medicine. The term has been applied to different dosing strategies aimed at improving outcomes and safety in complex patients displaying substantial interindividual variability in drug exposure and response. Depending on their degree of individualization, various “precision dosing methods” result in dosing recommendations for patient subgroups based on specific indications, genotypes, or patient characteristics like renal function, and/or in more individualized dosing based on measurements obtained during drug treatment, for example, drug concentrations from therapeutic drug monitoring (TDM). In complex situations in which target effect measurement and data interpretation are not straightforward, multiple pieces rather than a single pieces of information are ideally combined for precision dosing, requiring sophisticated predictive models.</p><p>Over the past 5–10 years, precision dosing activities, ranging from dried blood spot analyses of plasma drug concentrations to novel models and educational initiatives fostering better collaboration, have surged, with the goals of benefiting patients, aiding prescribers, saving money, and supporting the development of difficult-to-use drugs. This perspective describes recent advances that address five major challenges of precision dosing (<b>Figure</b> 1), followed by a summary of other challenges with slow progress.</p><p>There are strong economic and logistical reasons to limit the number of test doses studied in clinical development. Despite these challenges, precision dosing may be invaluable in tackling complex drug development scenarios, such as for (1) drugs with narrow therapeutic windows, (2) drugs that can lead to severe adverse effects at otherwise typical doses, (3) drugs used for conditions like cancer that carry serious consequences if undertreated, (4) drugs for treating rare, severe, and progressive diseases, and (5) drugs requiring invasive administration routes, for example, intravitreal or intrathecal.<span><sup>1</sup></span></p><p>Regulatory support is variable, but a successful example of pharma-regulatory collaboration supporting precision dosing is MyPKFit®, a clinical decision support (CDS) tool approved alongside recombinant factor VIII that personalizes dosing in hemophilia A. Also, the ophthalmologic drug faricimab was developed with a precision dosing arm in all four of its pivotal clinical trials, covering two indications, that is, neovascular age-related macular degeneration and diabetic macular edema. Personalized treatment with faricimab was approved, with dosing interval individualization according to disease activity such as visual outcomes.<span><sup>1</sup></span></p><p>Generating clinical trial evidence for precision dosing poses a significant challenge with much progress in recent years. As confidence in dose predictions increases (Challenge 4), incorporating MIPD into prospective clinical trials, such as concentration-controlled or effect-controlled trials, is becoming more common.</p><p>Phase II and III studies with individualized dosing arms rather than fixed dosing arms facilitate the exploration of wider and more nuanced doses, resulting in the approval of dose ranges, and subsequently reduced necessity for off-label dosing. Clinical trials of GLP-1 agonists use this approach because there is a fine balance between efficacy and gastrointestinal intolerance.<span><sup>2</sup></span></p><p>In 2021, the FDA's Oncology Center of Excellence initiated Project Optimus to reform the dose selection paradigm in oncology drug development. Project Optimus's primary goal is to ensure that new cancer drugs are developed with optimal dosing strategies by leveraging modern clinical trial designs and more adaptable, patient-centered approaches to dosing – instead of the conventional maximum tolerated dose approach – that consider individual variability and the unique characteristics of the respective cancer type.</p><p>Substantial portions of pharmacokinetic-pharmacodynamic (PK-PD) variability remain unknown for many drugs. Efforts to further understand disease heterogeneity and variability in drug responses, even among patients with comparable drug exposures, have significantly increased in the last decade with the discovery of novel biomarkers and the development of new, more sensitive analysis methods.</p><p>For certain drugs, TDM utilizing microsampling devices – allowing dried blood spot collection at home and delivery to a laboratory for concentration testing – is feasible.<span><sup>3</sup></span> Furthermore, recent advances in biosensor technology have improved the ability to measure drug concentrations directly and non-invasively.<span><sup>4</sup></span> This extends to biomarker monitoring, exemplified by the boom in continuous blood glucose monitoring patches that provide feedback on antidiabetic drug responses.</p><p>Wearable devices further allow noninvasive and real-time collection of various vital signs and health-related data, including heart rate, blood pressure, and other biomarkers. Considering these data in MIPD systems holds promise for precision dosing, not only relying on PK parameters (e.g., trough concentrations or area under the plasma drug concentration-time curve results, AUC), but also leveraging novel PD biomarkers and clinical- or patient-related treatment outcomes. Quantitative systems pharmacology and disease modeling can provide a mechanistic framework to integrate PD biomarkers that predict disease progression, treatment response, and drug safety.<span><sup>5</sup></span></p><p>Finally, with the improved ability to collect and securely store extensive amounts of data from both clinical trial and real-world settings, artificial intelligence and machine learning (AI-ML) are growing in importance for identifying patterns of covariates associated with certain clinical outcomes, which could ultimately inform optimal dosing strategies for individual patients.<span><sup>1</sup></span></p><p>Recent technological advancements and research efforts have significantly improved the feasibility of precision dosing in highly complex patients. Evolving MIPD approaches now offer a framework to simultaneously integrate several patient-, drug-, and disease-related covariates known to influence drug exposures and responses.</p><p>A MIPD approach with proof-of-concept data that is yet to be applied prospectively in the clinic is physiologically-based pharmacokinetic (PBPK) modeling and simulation. The terms “virtual twins” and “digital twins” have been coined to describe this type of MIPD, which simulates an individual's PK profile based on their physiology and health status. It is especially appealing for drugs with established target exposure ranges and for special, understudied populations of patients (e.g., children, pregnant women, and lactating mothers) in whom dosing recommendations are unavailable, or when population PK models to guide dosing do not exist.</p><p>AI-ML methods are increasingly studied in precision dosing to predict drug exposure, the incidence of adverse drug reactions, efficacy, or other outcomes.<span><sup>6</sup></span> Examples of pioneering work include the utilization of extreme gradient boosting (XGBoost) models to predict exposures to tacrolimus and mycophenolic acid in support of precision dosing of immunosuppressants.<span><sup>7</sup></span> Additionally, hybrid ML-PK-PD methods, merging AI-ML with traditional pharmacometric approaches, have been investigated to support MIPD systems. A recent study demonstrated that simulation-based data augmentation and enrichment of ML model features with PK-PD model predictions enhanced the predictive ability of the ML model in forecasting chemotherapy-induced neutropenia.<span><sup>8</sup></span> Continuous learning and other approaches to refine PK-PD model parameters and continuously update models used for MIPD have been proposed, and AI-ML could facilitate these processes automatically or semi-automatically as new clinical data are collected through electronic health records (EHRs). In addition, reinforcement learning constitutes a promising approach to enhancing MIPD with the capability of continuous learning.</p><p>Complex dosing and monitoring are difficult to implement, and more advanced precision dosing approaches, including pharmacogenomic (PGx)-guided dosing, are often limited to a few specialties, e.g. hematology, oncology, or pediatrics.<span><sup>9</sup></span> To address clinical implementation, major steps forward in developing user-friendly precision dosing solutions have been achieved in recent years. Furthermore, the successful establishment of precision dosing CDS tools encompasses strategic planning, seamless integration into existing workflows, and continuous improvement. Coupled with the adoption of FHIR (Fast Healthcare Interoperability Resources) standards, these systems can be integrated with major EHRs, paving the way for broader adoption. Companies such as InsightRx and DoseMeRx have successfully demonstrated these integration capabilities for MIPD of approved drugs requiring TDM, including various antimicrobials, immunosuppressants, and anticancer drugs. Moreover, the scope of data within EHRs has been broadening to include a variety of relevant biomarkers and genetic information, facilitating PGx-guided dosing.</p><p>Professional societies are increasingly taking the lead on precision dosing guidelines. This sets the precedent that adherence to drug labeling is softened by professional consensus. Vancomycin dosing and TDM guidelines in 2020 marked a significant milestone in this regard, catalyzing several health systems to implement MIPD strategies aimed at achieving targeted AUC metrics.<span><sup>10</sup></span></p><p>Diverse types of information can inform precision dosing, though necessitating efficient and safe integration from different data sources. The importance of data sharing, while adhering to data protection and privacy regulations, and sometimes with competing commercial interests (e.g., pathology providers), is not to be underestimated, and must be solved for more complex precision dosing approaches to succeed.</p><p>Once precision dosing has been implemented in practice, clinical trials and real-world evidence investigating its benefits over standard approaches are crucial to increase acceptance and foster more widespread adoption. Challenges of conducting such studies include the selection of appropriate precision dosing targets, appropriate end points (e.g., clinical- and patient-reported outcomes), and timing.</p><p>Precision dosing requires additional ethical and legal considerations, including consent from patients and legal protection for prescribers when doses different from those approved are used in the spirit of beneficence. This would be facilitated when guidelines are available from professional societies (Challenge 5).</p><p>Finally, novel reimbursement models for drug therapies are required to encourage precision dosing in drug development and clinical practice. For example, therapy prices independent of the prescribed dose, including outcome-based reimbursement, would accelerate the adoption of precision dosing.</p><p>This perspective emphasizes recent advances in precision dosing and outlines some outstanding opportunities. As precision dosing evolves, greater integration into drug development and clinical practice holds promise to significantly advance personalized medicine, offering more tailored, effective, and safe drug treatments for more patients.</p><p>No funding was received for this work.</p><p>IKM, TM, and TMP declare no conflicts of interest. RWP holds stock in and receives compensation from F Hoffmann la Roche. SG is employed by InsightRx, which produces model-informed precision dosing clinical decision support tools. As an Associate Editor for Clinical Pharmacology & Therapeutics, Iris Minichmayr was not involved in the review or decision process for this paper.</p>\",\"PeriodicalId\":153,\"journal\":{\"name\":\"Clinical Pharmacology & Therapeutics\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":6.3000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3365\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacology & Therapeutics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cpt.3365\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacology & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cpt.3365","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Recent Advances Addressing the Challenges of Precision Dosing
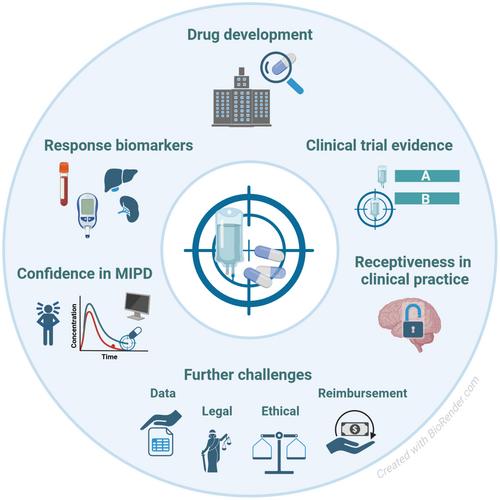
Precision dosing can improve drug therapy in complex, critically ill, and chronically ill patient populations who exhibit vast interindividual variabilities in exposures and responses. This perspective outlines five major challenges in precision dosing and highlights their recent progress: (1) application in drug development, (2) improved clinical trials, (3) usefulness of response biomarkers, (4) confidence in model-informed precision dosing, and (5) receptiveness in clinical practice. Many outstanding opportunities in precision dosing remain within regulatory frameworks, data integration and protection, ethics, and reimbursement strategies.
Precision dosing is a foundational pillar of personalized medicine. The term has been applied to different dosing strategies aimed at improving outcomes and safety in complex patients displaying substantial interindividual variability in drug exposure and response. Depending on their degree of individualization, various “precision dosing methods” result in dosing recommendations for patient subgroups based on specific indications, genotypes, or patient characteristics like renal function, and/or in more individualized dosing based on measurements obtained during drug treatment, for example, drug concentrations from therapeutic drug monitoring (TDM). In complex situations in which target effect measurement and data interpretation are not straightforward, multiple pieces rather than a single pieces of information are ideally combined for precision dosing, requiring sophisticated predictive models.
Over the past 5–10 years, precision dosing activities, ranging from dried blood spot analyses of plasma drug concentrations to novel models and educational initiatives fostering better collaboration, have surged, with the goals of benefiting patients, aiding prescribers, saving money, and supporting the development of difficult-to-use drugs. This perspective describes recent advances that address five major challenges of precision dosing (Figure 1), followed by a summary of other challenges with slow progress.
There are strong economic and logistical reasons to limit the number of test doses studied in clinical development. Despite these challenges, precision dosing may be invaluable in tackling complex drug development scenarios, such as for (1) drugs with narrow therapeutic windows, (2) drugs that can lead to severe adverse effects at otherwise typical doses, (3) drugs used for conditions like cancer that carry serious consequences if undertreated, (4) drugs for treating rare, severe, and progressive diseases, and (5) drugs requiring invasive administration routes, for example, intravitreal or intrathecal.1
Regulatory support is variable, but a successful example of pharma-regulatory collaboration supporting precision dosing is MyPKFit®, a clinical decision support (CDS) tool approved alongside recombinant factor VIII that personalizes dosing in hemophilia A. Also, the ophthalmologic drug faricimab was developed with a precision dosing arm in all four of its pivotal clinical trials, covering two indications, that is, neovascular age-related macular degeneration and diabetic macular edema. Personalized treatment with faricimab was approved, with dosing interval individualization according to disease activity such as visual outcomes.1
Generating clinical trial evidence for precision dosing poses a significant challenge with much progress in recent years. As confidence in dose predictions increases (Challenge 4), incorporating MIPD into prospective clinical trials, such as concentration-controlled or effect-controlled trials, is becoming more common.
Phase II and III studies with individualized dosing arms rather than fixed dosing arms facilitate the exploration of wider and more nuanced doses, resulting in the approval of dose ranges, and subsequently reduced necessity for off-label dosing. Clinical trials of GLP-1 agonists use this approach because there is a fine balance between efficacy and gastrointestinal intolerance.2
In 2021, the FDA's Oncology Center of Excellence initiated Project Optimus to reform the dose selection paradigm in oncology drug development. Project Optimus's primary goal is to ensure that new cancer drugs are developed with optimal dosing strategies by leveraging modern clinical trial designs and more adaptable, patient-centered approaches to dosing – instead of the conventional maximum tolerated dose approach – that consider individual variability and the unique characteristics of the respective cancer type.
Substantial portions of pharmacokinetic-pharmacodynamic (PK-PD) variability remain unknown for many drugs. Efforts to further understand disease heterogeneity and variability in drug responses, even among patients with comparable drug exposures, have significantly increased in the last decade with the discovery of novel biomarkers and the development of new, more sensitive analysis methods.
For certain drugs, TDM utilizing microsampling devices – allowing dried blood spot collection at home and delivery to a laboratory for concentration testing – is feasible.3 Furthermore, recent advances in biosensor technology have improved the ability to measure drug concentrations directly and non-invasively.4 This extends to biomarker monitoring, exemplified by the boom in continuous blood glucose monitoring patches that provide feedback on antidiabetic drug responses.
Wearable devices further allow noninvasive and real-time collection of various vital signs and health-related data, including heart rate, blood pressure, and other biomarkers. Considering these data in MIPD systems holds promise for precision dosing, not only relying on PK parameters (e.g., trough concentrations or area under the plasma drug concentration-time curve results, AUC), but also leveraging novel PD biomarkers and clinical- or patient-related treatment outcomes. Quantitative systems pharmacology and disease modeling can provide a mechanistic framework to integrate PD biomarkers that predict disease progression, treatment response, and drug safety.5
Finally, with the improved ability to collect and securely store extensive amounts of data from both clinical trial and real-world settings, artificial intelligence and machine learning (AI-ML) are growing in importance for identifying patterns of covariates associated with certain clinical outcomes, which could ultimately inform optimal dosing strategies for individual patients.1
Recent technological advancements and research efforts have significantly improved the feasibility of precision dosing in highly complex patients. Evolving MIPD approaches now offer a framework to simultaneously integrate several patient-, drug-, and disease-related covariates known to influence drug exposures and responses.
A MIPD approach with proof-of-concept data that is yet to be applied prospectively in the clinic is physiologically-based pharmacokinetic (PBPK) modeling and simulation. The terms “virtual twins” and “digital twins” have been coined to describe this type of MIPD, which simulates an individual's PK profile based on their physiology and health status. It is especially appealing for drugs with established target exposure ranges and for special, understudied populations of patients (e.g., children, pregnant women, and lactating mothers) in whom dosing recommendations are unavailable, or when population PK models to guide dosing do not exist.
AI-ML methods are increasingly studied in precision dosing to predict drug exposure, the incidence of adverse drug reactions, efficacy, or other outcomes.6 Examples of pioneering work include the utilization of extreme gradient boosting (XGBoost) models to predict exposures to tacrolimus and mycophenolic acid in support of precision dosing of immunosuppressants.7 Additionally, hybrid ML-PK-PD methods, merging AI-ML with traditional pharmacometric approaches, have been investigated to support MIPD systems. A recent study demonstrated that simulation-based data augmentation and enrichment of ML model features with PK-PD model predictions enhanced the predictive ability of the ML model in forecasting chemotherapy-induced neutropenia.8 Continuous learning and other approaches to refine PK-PD model parameters and continuously update models used for MIPD have been proposed, and AI-ML could facilitate these processes automatically or semi-automatically as new clinical data are collected through electronic health records (EHRs). In addition, reinforcement learning constitutes a promising approach to enhancing MIPD with the capability of continuous learning.
Complex dosing and monitoring are difficult to implement, and more advanced precision dosing approaches, including pharmacogenomic (PGx)-guided dosing, are often limited to a few specialties, e.g. hematology, oncology, or pediatrics.9 To address clinical implementation, major steps forward in developing user-friendly precision dosing solutions have been achieved in recent years. Furthermore, the successful establishment of precision dosing CDS tools encompasses strategic planning, seamless integration into existing workflows, and continuous improvement. Coupled with the adoption of FHIR (Fast Healthcare Interoperability Resources) standards, these systems can be integrated with major EHRs, paving the way for broader adoption. Companies such as InsightRx and DoseMeRx have successfully demonstrated these integration capabilities for MIPD of approved drugs requiring TDM, including various antimicrobials, immunosuppressants, and anticancer drugs. Moreover, the scope of data within EHRs has been broadening to include a variety of relevant biomarkers and genetic information, facilitating PGx-guided dosing.
Professional societies are increasingly taking the lead on precision dosing guidelines. This sets the precedent that adherence to drug labeling is softened by professional consensus. Vancomycin dosing and TDM guidelines in 2020 marked a significant milestone in this regard, catalyzing several health systems to implement MIPD strategies aimed at achieving targeted AUC metrics.10
Diverse types of information can inform precision dosing, though necessitating efficient and safe integration from different data sources. The importance of data sharing, while adhering to data protection and privacy regulations, and sometimes with competing commercial interests (e.g., pathology providers), is not to be underestimated, and must be solved for more complex precision dosing approaches to succeed.
Once precision dosing has been implemented in practice, clinical trials and real-world evidence investigating its benefits over standard approaches are crucial to increase acceptance and foster more widespread adoption. Challenges of conducting such studies include the selection of appropriate precision dosing targets, appropriate end points (e.g., clinical- and patient-reported outcomes), and timing.
Precision dosing requires additional ethical and legal considerations, including consent from patients and legal protection for prescribers when doses different from those approved are used in the spirit of beneficence. This would be facilitated when guidelines are available from professional societies (Challenge 5).
Finally, novel reimbursement models for drug therapies are required to encourage precision dosing in drug development and clinical practice. For example, therapy prices independent of the prescribed dose, including outcome-based reimbursement, would accelerate the adoption of precision dosing.
This perspective emphasizes recent advances in precision dosing and outlines some outstanding opportunities. As precision dosing evolves, greater integration into drug development and clinical practice holds promise to significantly advance personalized medicine, offering more tailored, effective, and safe drug treatments for more patients.
No funding was received for this work.
IKM, TM, and TMP declare no conflicts of interest. RWP holds stock in and receives compensation from F Hoffmann la Roche. SG is employed by InsightRx, which produces model-informed precision dosing clinical decision support tools. As an Associate Editor for Clinical Pharmacology & Therapeutics, Iris Minichmayr was not involved in the review or decision process for this paper.
期刊介绍:
Clinical Pharmacology & Therapeutics (CPT) is the authoritative cross-disciplinary journal in experimental and clinical medicine devoted to publishing advances in the nature, action, efficacy, and evaluation of therapeutics. CPT welcomes original Articles in the emerging areas of translational, predictive and personalized medicine; new therapeutic modalities including gene and cell therapies; pharmacogenomics, proteomics and metabolomics; bioinformation and applied systems biology complementing areas of pharmacokinetics and pharmacodynamics, human investigation and clinical trials, pharmacovigilence, pharmacoepidemiology, pharmacometrics, and population pharmacology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


