{"title":"在 COVID-19 大流行期间,社区中扑热息痛治疗失误率上升","authors":"Nicole O'Shea BPharm, MClinPharm, MSHP, GradCertPharmPrac, GradCertHlthMgmt, FANZCAP (Tox, MedSafety), Rohan A. Elliott BPharm, BpharmSc(Hons), MClinPharm, PhD, FSHP, FANZCAP (GeriMed, Research), Anselm Wong MBBS, DipTox, PhD, FACEM, FACMT, FAACT, FEAPCCT","doi":"10.1002/jppr.1936","DOIUrl":null,"url":null,"abstract":"<p>Treatment guidelines for COVID-19 recommend basic analgesics/antipyretics such as paracetamol.<span><sup>1</sup></span> Paracetamol therapeutic errors are associated with morbidity and mortality.<span><sup>2</sup></span> The Victorian Poisons Information Centre (VPIC), the statewide poisons centre for Victoria, Australia, receives calls from members of the public for advice regarding errors made with medicines. Paracetamol therapeutic errors are usually accidental overdoses (e.g. double-dose, maximum daily dose exceeded, incorrectly measured liquid paracetamol, or use of two paracetamol-containing medicines). The aim of this research was to explore the impact of the COVID-19 pandemic on the number of paracetamol therapeutic error cases in the community (outside of hospitals) that were reported to VPIC.</p><p>Call records were extracted from the VPIC database from 1 July 2017 to 30 June 2022 (approximately 2.5 years before and after the first cases of COVID-19 in Victoria). Retrospectively, records were reviewed where callers reported a therapeutic error with any form of paracetamol that occurred in an adult or child in the home or community.</p><p>In the 2.5 years prior to the pandemic there was an average of 120 (standard deviation [SD] 21) paracetamol therapeutic error cases per month. In the 2.5 years from January 2020 there was an average of 116 (SD 33) cases per month, but case numbers varied as the Victorian population went into and out of lockdown (lockdowns were a stay-at-home order to reduce the spread of COVID-19). During the first two Melbourne lockdowns, which occurred between 31 March 2020–12 May 2020 and 9 July 2020–27 October 2020,<span><sup>3</sup></span> the average number of paracetamol therapeutic error cases per month fell to 60 (SD 19) and 80 (SD 5) per month, respectively. During this time, COVID-19 cases remained low (Figure 1).<span><sup>4</sup></span> When the number of COVID-19 cases rose in the second half of 2021, the average number of paracetamol therapeutic error cases per month increased.<span><sup>4</sup></span> The mean number of cases after lockdowns ended (22 October 2021–30 June 2022) was 145 per month compared to 120 per month pre-pandemic (p < 0.001).</p><p>In reviewing cases related to paediatrics and adolescents (defined in the database as people ≤19 years of age) prior to COVID-19, the average number of therapeutic error cases was 62.66 (SD 13) per month. After the COVID-19 lockdown periods, the average number of therapeutic error cases per month increased to 80 (SD 26, p < 0.001).</p><p>The lower number of paracetamol therapeutic error cases reported to VPIC during the first two lockdowns could be explained by an overall reduction in viral illness due to prolonged lockdowns and improved infection control (e.g. social distancing, face masks, improved hand hygiene).<span><sup>5</sup></span> The statistically significant increase in paracetamol therapeutic errors in the post-lockdown period, compared to pre-COVID-19, may be due to the increased paracetamol use in the community due to high COVID-19 case numbers and other viral illnesses such as influenza.</p><p>A limitation of the data is that only cases reported to VPIC were included. We do not have data on how many patients experienced toxicity from their overdose, but the numbers of patients referred to hospital or in hospital are included in Figure 1.</p><p>Callers were not routinely asked about what had caused the paracetamol therapeutic error. Anecdotally, VPIC staff noted that people with COVID-19 symptoms often reported taking paracetamol 4-hourly, without regard to the maximum daily dose. Some callers reported that they were instructed by a health professional to take paracetamol 4-hourly. It is important that the public and health professionals understand the risks associated with paracetamol and how to use paracetamol safely in the management of acute viral illnesses.</p><p>None.</p><p>Rohan A. Elliot was the former Geriatric Therapeutics Review Editor for the <i>Journal of Pharmacy Practice and Research</i> and an author of this article. He was excluded from editorial decision-making related to the acceptance and publication of this article. The remaining authors declare that they have no conflicts of interest.</p><p><b>Nicole O'Shea:</b> Writing – original draft; project administration; formal analysis; investigation; methodology. <b>Rohan A. Elliott:</b> Formal analysis; validation; writing – review and editing; supervision; data curation. <b>Anselm Wong:</b> Project administration; writing – review and editing; validation; resources; supervision.</p><p>Ethical approval was granted by the Austin Health Human Research Ethics Committee (Reference no: HREC/67865/Austin-2020) and the study conforms to the <i>Australian National Statement on Ethical Conduct in Human Research</i>.</p><p>This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.</p>","PeriodicalId":16795,"journal":{"name":"Journal of Pharmacy Practice and Research","volume":"54 5","pages":"436-438"},"PeriodicalIF":1.0000,"publicationDate":"2024-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jppr.1936","citationCount":"0","resultStr":"{\"title\":\"Rise in paracetamol therapeutic errors in the community during the COVID-19 pandemic\",\"authors\":\"Nicole O'Shea BPharm, MClinPharm, MSHP, GradCertPharmPrac, GradCertHlthMgmt, FANZCAP (Tox, MedSafety), Rohan A. Elliott BPharm, BpharmSc(Hons), MClinPharm, PhD, FSHP, FANZCAP (GeriMed, Research), Anselm Wong MBBS, DipTox, PhD, FACEM, FACMT, FAACT, FEAPCCT\",\"doi\":\"10.1002/jppr.1936\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Treatment guidelines for COVID-19 recommend basic analgesics/antipyretics such as paracetamol.<span><sup>1</sup></span> Paracetamol therapeutic errors are associated with morbidity and mortality.<span><sup>2</sup></span> The Victorian Poisons Information Centre (VPIC), the statewide poisons centre for Victoria, Australia, receives calls from members of the public for advice regarding errors made with medicines. Paracetamol therapeutic errors are usually accidental overdoses (e.g. double-dose, maximum daily dose exceeded, incorrectly measured liquid paracetamol, or use of two paracetamol-containing medicines). The aim of this research was to explore the impact of the COVID-19 pandemic on the number of paracetamol therapeutic error cases in the community (outside of hospitals) that were reported to VPIC.</p><p>Call records were extracted from the VPIC database from 1 July 2017 to 30 June 2022 (approximately 2.5 years before and after the first cases of COVID-19 in Victoria). Retrospectively, records were reviewed where callers reported a therapeutic error with any form of paracetamol that occurred in an adult or child in the home or community.</p><p>In the 2.5 years prior to the pandemic there was an average of 120 (standard deviation [SD] 21) paracetamol therapeutic error cases per month. In the 2.5 years from January 2020 there was an average of 116 (SD 33) cases per month, but case numbers varied as the Victorian population went into and out of lockdown (lockdowns were a stay-at-home order to reduce the spread of COVID-19). During the first two Melbourne lockdowns, which occurred between 31 March 2020–12 May 2020 and 9 July 2020–27 October 2020,<span><sup>3</sup></span> the average number of paracetamol therapeutic error cases per month fell to 60 (SD 19) and 80 (SD 5) per month, respectively. During this time, COVID-19 cases remained low (Figure 1).<span><sup>4</sup></span> When the number of COVID-19 cases rose in the second half of 2021, the average number of paracetamol therapeutic error cases per month increased.<span><sup>4</sup></span> The mean number of cases after lockdowns ended (22 October 2021–30 June 2022) was 145 per month compared to 120 per month pre-pandemic (p < 0.001).</p><p>In reviewing cases related to paediatrics and adolescents (defined in the database as people ≤19 years of age) prior to COVID-19, the average number of therapeutic error cases was 62.66 (SD 13) per month. After the COVID-19 lockdown periods, the average number of therapeutic error cases per month increased to 80 (SD 26, p < 0.001).</p><p>The lower number of paracetamol therapeutic error cases reported to VPIC during the first two lockdowns could be explained by an overall reduction in viral illness due to prolonged lockdowns and improved infection control (e.g. social distancing, face masks, improved hand hygiene).<span><sup>5</sup></span> The statistically significant increase in paracetamol therapeutic errors in the post-lockdown period, compared to pre-COVID-19, may be due to the increased paracetamol use in the community due to high COVID-19 case numbers and other viral illnesses such as influenza.</p><p>A limitation of the data is that only cases reported to VPIC were included. We do not have data on how many patients experienced toxicity from their overdose, but the numbers of patients referred to hospital or in hospital are included in Figure 1.</p><p>Callers were not routinely asked about what had caused the paracetamol therapeutic error. Anecdotally, VPIC staff noted that people with COVID-19 symptoms often reported taking paracetamol 4-hourly, without regard to the maximum daily dose. Some callers reported that they were instructed by a health professional to take paracetamol 4-hourly. It is important that the public and health professionals understand the risks associated with paracetamol and how to use paracetamol safely in the management of acute viral illnesses.</p><p>None.</p><p>Rohan A. Elliot was the former Geriatric Therapeutics Review Editor for the <i>Journal of Pharmacy Practice and Research</i> and an author of this article. He was excluded from editorial decision-making related to the acceptance and publication of this article. The remaining authors declare that they have no conflicts of interest.</p><p><b>Nicole O'Shea:</b> Writing – original draft; project administration; formal analysis; investigation; methodology. <b>Rohan A. Elliott:</b> Formal analysis; validation; writing – review and editing; supervision; data curation. <b>Anselm Wong:</b> Project administration; writing – review and editing; validation; resources; supervision.</p><p>Ethical approval was granted by the Austin Health Human Research Ethics Committee (Reference no: HREC/67865/Austin-2020) and the study conforms to the <i>Australian National Statement on Ethical Conduct in Human Research</i>.</p><p>This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.</p>\",\"PeriodicalId\":16795,\"journal\":{\"name\":\"Journal of Pharmacy Practice and Research\",\"volume\":\"54 5\",\"pages\":\"436-438\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jppr.1936\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmacy Practice and Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jppr.1936\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmacy Practice and Research","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jppr.1936","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Rise in paracetamol therapeutic errors in the community during the COVID-19 pandemic
Treatment guidelines for COVID-19 recommend basic analgesics/antipyretics such as paracetamol.1 Paracetamol therapeutic errors are associated with morbidity and mortality.2 The Victorian Poisons Information Centre (VPIC), the statewide poisons centre for Victoria, Australia, receives calls from members of the public for advice regarding errors made with medicines. Paracetamol therapeutic errors are usually accidental overdoses (e.g. double-dose, maximum daily dose exceeded, incorrectly measured liquid paracetamol, or use of two paracetamol-containing medicines). The aim of this research was to explore the impact of the COVID-19 pandemic on the number of paracetamol therapeutic error cases in the community (outside of hospitals) that were reported to VPIC.
Call records were extracted from the VPIC database from 1 July 2017 to 30 June 2022 (approximately 2.5 years before and after the first cases of COVID-19 in Victoria). Retrospectively, records were reviewed where callers reported a therapeutic error with any form of paracetamol that occurred in an adult or child in the home or community.
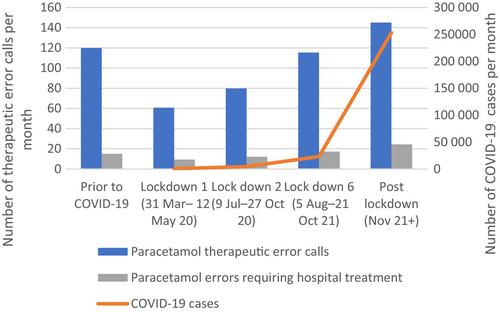
In the 2.5 years prior to the pandemic there was an average of 120 (standard deviation [SD] 21) paracetamol therapeutic error cases per month. In the 2.5 years from January 2020 there was an average of 116 (SD 33) cases per month, but case numbers varied as the Victorian population went into and out of lockdown (lockdowns were a stay-at-home order to reduce the spread of COVID-19). During the first two Melbourne lockdowns, which occurred between 31 March 2020–12 May 2020 and 9 July 2020–27 October 2020,3 the average number of paracetamol therapeutic error cases per month fell to 60 (SD 19) and 80 (SD 5) per month, respectively. During this time, COVID-19 cases remained low (Figure 1).4 When the number of COVID-19 cases rose in the second half of 2021, the average number of paracetamol therapeutic error cases per month increased.4 The mean number of cases after lockdowns ended (22 October 2021–30 June 2022) was 145 per month compared to 120 per month pre-pandemic (p < 0.001).
In reviewing cases related to paediatrics and adolescents (defined in the database as people ≤19 years of age) prior to COVID-19, the average number of therapeutic error cases was 62.66 (SD 13) per month. After the COVID-19 lockdown periods, the average number of therapeutic error cases per month increased to 80 (SD 26, p < 0.001).
The lower number of paracetamol therapeutic error cases reported to VPIC during the first two lockdowns could be explained by an overall reduction in viral illness due to prolonged lockdowns and improved infection control (e.g. social distancing, face masks, improved hand hygiene).5 The statistically significant increase in paracetamol therapeutic errors in the post-lockdown period, compared to pre-COVID-19, may be due to the increased paracetamol use in the community due to high COVID-19 case numbers and other viral illnesses such as influenza.
A limitation of the data is that only cases reported to VPIC were included. We do not have data on how many patients experienced toxicity from their overdose, but the numbers of patients referred to hospital or in hospital are included in Figure 1.
Callers were not routinely asked about what had caused the paracetamol therapeutic error. Anecdotally, VPIC staff noted that people with COVID-19 symptoms often reported taking paracetamol 4-hourly, without regard to the maximum daily dose. Some callers reported that they were instructed by a health professional to take paracetamol 4-hourly. It is important that the public and health professionals understand the risks associated with paracetamol and how to use paracetamol safely in the management of acute viral illnesses.
None.
Rohan A. Elliot was the former Geriatric Therapeutics Review Editor for the Journal of Pharmacy Practice and Research and an author of this article. He was excluded from editorial decision-making related to the acceptance and publication of this article. The remaining authors declare that they have no conflicts of interest.
Nicole O'Shea: Writing – original draft; project administration; formal analysis; investigation; methodology. Rohan A. Elliott: Formal analysis; validation; writing – review and editing; supervision; data curation. Anselm Wong: Project administration; writing – review and editing; validation; resources; supervision.
Ethical approval was granted by the Austin Health Human Research Ethics Committee (Reference no: HREC/67865/Austin-2020) and the study conforms to the Australian National Statement on Ethical Conduct in Human Research.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
期刊介绍:
The purpose of this document is to describe the structure, function and operations of the Journal of Pharmacy Practice and Research, the official journal of the Society of Hospital Pharmacists of Australia (SHPA). It is owned, published by and copyrighted to SHPA. However, the Journal is to some extent unique within SHPA in that it ‘…has complete editorial freedom in terms of content and is not under the direction of the Society or its Council in such matters…’. This statement, originally based on a Role Statement for the Editor-in-Chief 1993, is also based on the definition of ‘editorial independence’ from the World Association of Medical Editors and adopted by the International Committee of Medical Journal Editors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


