{"title":"视频辅助胸腔手术指导下早期排出创伤性血气胸的效果:一级创伤中心的随机试点研究。","authors":"Abhinav Kumar, Dinesh Gora, Dinesh Bagaria, Pratyusha Priyadarshini, Narendra Choudhary, Amit Priyadarshi, Sahil Gupta, Junaid Alam, Amit Gupta, Biplab Mishra, Subodh Kumar, Sushma Sagar","doi":"10.4103/jets.jets_132_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Traumatic hemothorax is accounted for about 20% of traumatic chest injuries. Although majority can be managed with the timely placement of intercostal tube (ICT) drainage, the remaining pose a challenge owing to high complication rates associated with retained hemothorax. Although various treatment modalities including intrapleural instillation of fibrinolytics, radioimage guided drainage, VATS guided evacuation and thoractomy do exist to address the retained hemothorax, but indications along with timing to employ a specific treatment option is still unclear and ambiguous.</p><p><strong>Methods: </strong>Patient with residual hemothorax (>200 mL) on ultrasonography after 48 h of indwelling ICT was randomized into either early video-assisted thoracic surgery (VATS) or conventional approach cohort. Early VATS cohort was subjected to video-assisted thoracoscopic evacuation of undrained blood along with normal saline irrigation and ICT placement. The conventional cohort underwent intrapleural thrombolytic instillation for 3 consecutive days. The outcome measures were the duration of indwelling ICT, removal rate of tube thoracostomy, length of hospital stay, duration of intensive care unit (ICU) monitoring, need for mechanical ventilation, incidence of pulmonary and pleural complications, and requirement of additional intervention to address undrained hemothorax and mortality rate.</p><p><strong>Results: </strong>The early VATS cohort had shorter length of hospital stay (7.50 ± 0.85 vs. 9.50 ± 3.03, <i>P</i> = 0.060), reduced duration of indwelling ICT (6.70 ± 1.25 vs. 8.30 ± 2.91, <i>P</i> = 0.127) with higher rate of tube thoracostomy removal (70% vs. 30%, <i>P</i> = 0.003) and lesser need of additional interventions (0% vs. 30%, <i>P</i> = 0.105). Thoracotomy (3 patients) and image-guided drainage (4 patients) were additional interventions to address retained hemothorax in the conventional cohort. However, similar length of ventilator assistance (0.7 ± 0.48 vs. 0.60 ± 1.08, <i>P</i> = 0.791) and prolonged ICU monitoring (1.30 ± 1.06 vs. 0.90 ± 1.45, <i>P</i> = 0.490) was observed in early VATS cohort. Both the cohorts had no mortality.</p><p><strong>Conclusion: </strong>VATS-guided early evacuation of traumatic hemothorax is associated with shorter length of hospital stay along with abbreviated indwelling ICT duration, reduced incidence of complications, lesser readmissions, and improved rate of tube thoracostomy removal. However, the duration of ventilator requirement, ICU stay, and mortality remain unchanged.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"17 2","pages":"73-79"},"PeriodicalIF":0.7000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11279504/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of Video-assisted Thoracic Surgery-guided Early Evacuation of Traumatic Hemothorax: A Randomized Pilot Study at Level I Trauma Center.\",\"authors\":\"Abhinav Kumar, Dinesh Gora, Dinesh Bagaria, Pratyusha Priyadarshini, Narendra Choudhary, Amit Priyadarshi, Sahil Gupta, Junaid Alam, Amit Gupta, Biplab Mishra, Subodh Kumar, Sushma Sagar\",\"doi\":\"10.4103/jets.jets_132_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Traumatic hemothorax is accounted for about 20% of traumatic chest injuries. Although majority can be managed with the timely placement of intercostal tube (ICT) drainage, the remaining pose a challenge owing to high complication rates associated with retained hemothorax. Although various treatment modalities including intrapleural instillation of fibrinolytics, radioimage guided drainage, VATS guided evacuation and thoractomy do exist to address the retained hemothorax, but indications along with timing to employ a specific treatment option is still unclear and ambiguous.</p><p><strong>Methods: </strong>Patient with residual hemothorax (>200 mL) on ultrasonography after 48 h of indwelling ICT was randomized into either early video-assisted thoracic surgery (VATS) or conventional approach cohort. Early VATS cohort was subjected to video-assisted thoracoscopic evacuation of undrained blood along with normal saline irrigation and ICT placement. The conventional cohort underwent intrapleural thrombolytic instillation for 3 consecutive days. The outcome measures were the duration of indwelling ICT, removal rate of tube thoracostomy, length of hospital stay, duration of intensive care unit (ICU) monitoring, need for mechanical ventilation, incidence of pulmonary and pleural complications, and requirement of additional intervention to address undrained hemothorax and mortality rate.</p><p><strong>Results: </strong>The early VATS cohort had shorter length of hospital stay (7.50 ± 0.85 vs. 9.50 ± 3.03, <i>P</i> = 0.060), reduced duration of indwelling ICT (6.70 ± 1.25 vs. 8.30 ± 2.91, <i>P</i> = 0.127) with higher rate of tube thoracostomy removal (70% vs. 30%, <i>P</i> = 0.003) and lesser need of additional interventions (0% vs. 30%, <i>P</i> = 0.105). Thoracotomy (3 patients) and image-guided drainage (4 patients) were additional interventions to address retained hemothorax in the conventional cohort. However, similar length of ventilator assistance (0.7 ± 0.48 vs. 0.60 ± 1.08, <i>P</i> = 0.791) and prolonged ICU monitoring (1.30 ± 1.06 vs. 0.90 ± 1.45, <i>P</i> = 0.490) was observed in early VATS cohort. Both the cohorts had no mortality.</p><p><strong>Conclusion: </strong>VATS-guided early evacuation of traumatic hemothorax is associated with shorter length of hospital stay along with abbreviated indwelling ICT duration, reduced incidence of complications, lesser readmissions, and improved rate of tube thoracostomy removal. However, the duration of ventilator requirement, ICU stay, and mortality remain unchanged.</p>\",\"PeriodicalId\":15692,\"journal\":{\"name\":\"Journal of Emergencies, Trauma, and Shock\",\"volume\":\"17 2\",\"pages\":\"73-79\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11279504/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Emergencies, Trauma, and Shock\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jets.jets_132_23\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_132_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Outcomes of Video-assisted Thoracic Surgery-guided Early Evacuation of Traumatic Hemothorax: A Randomized Pilot Study at Level I Trauma Center.
Introduction: Traumatic hemothorax is accounted for about 20% of traumatic chest injuries. Although majority can be managed with the timely placement of intercostal tube (ICT) drainage, the remaining pose a challenge owing to high complication rates associated with retained hemothorax. Although various treatment modalities including intrapleural instillation of fibrinolytics, radioimage guided drainage, VATS guided evacuation and thoractomy do exist to address the retained hemothorax, but indications along with timing to employ a specific treatment option is still unclear and ambiguous.
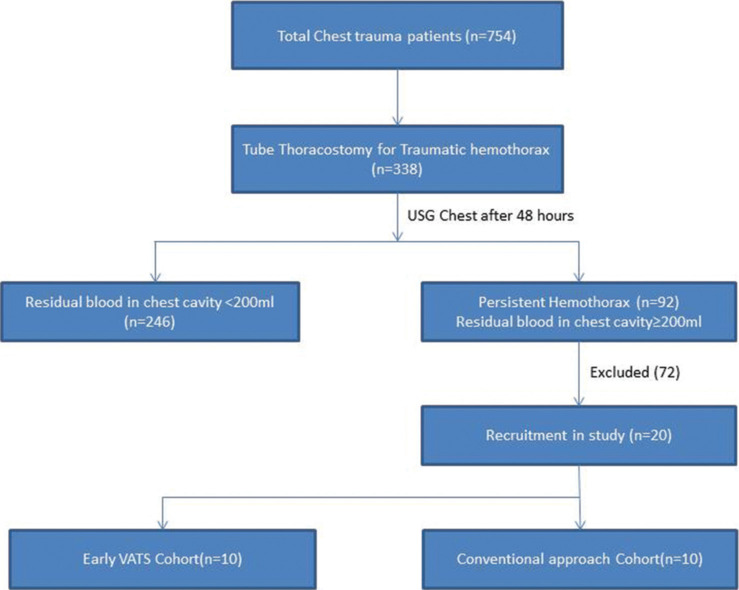
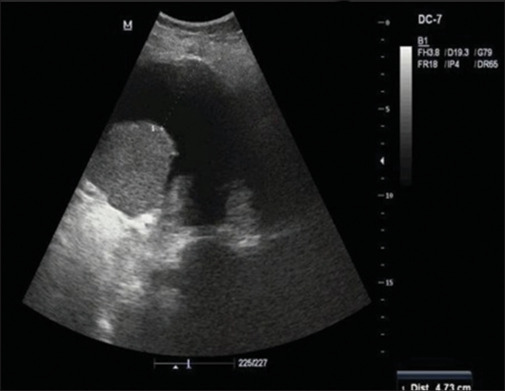
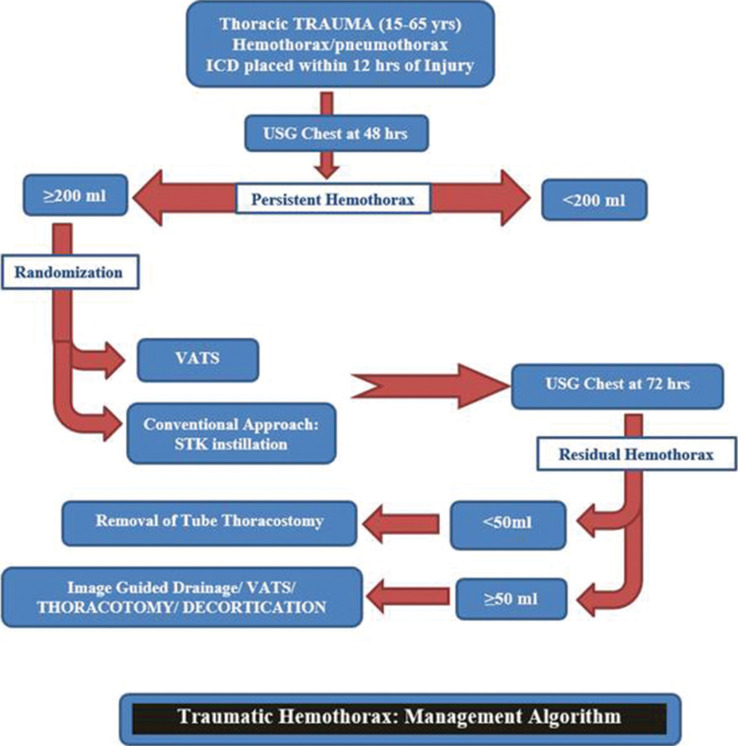
Methods: Patient with residual hemothorax (>200 mL) on ultrasonography after 48 h of indwelling ICT was randomized into either early video-assisted thoracic surgery (VATS) or conventional approach cohort. Early VATS cohort was subjected to video-assisted thoracoscopic evacuation of undrained blood along with normal saline irrigation and ICT placement. The conventional cohort underwent intrapleural thrombolytic instillation for 3 consecutive days. The outcome measures were the duration of indwelling ICT, removal rate of tube thoracostomy, length of hospital stay, duration of intensive care unit (ICU) monitoring, need for mechanical ventilation, incidence of pulmonary and pleural complications, and requirement of additional intervention to address undrained hemothorax and mortality rate.
Results: The early VATS cohort had shorter length of hospital stay (7.50 ± 0.85 vs. 9.50 ± 3.03, P = 0.060), reduced duration of indwelling ICT (6.70 ± 1.25 vs. 8.30 ± 2.91, P = 0.127) with higher rate of tube thoracostomy removal (70% vs. 30%, P = 0.003) and lesser need of additional interventions (0% vs. 30%, P = 0.105). Thoracotomy (3 patients) and image-guided drainage (4 patients) were additional interventions to address retained hemothorax in the conventional cohort. However, similar length of ventilator assistance (0.7 ± 0.48 vs. 0.60 ± 1.08, P = 0.791) and prolonged ICU monitoring (1.30 ± 1.06 vs. 0.90 ± 1.45, P = 0.490) was observed in early VATS cohort. Both the cohorts had no mortality.
Conclusion: VATS-guided early evacuation of traumatic hemothorax is associated with shorter length of hospital stay along with abbreviated indwelling ICT duration, reduced incidence of complications, lesser readmissions, and improved rate of tube thoracostomy removal. However, the duration of ventilator requirement, ICU stay, and mortality remain unchanged.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


