William Shippam, Simon Massey, Kathyrn Clark, Luc Saulnier, Anthony Chau
{"title":"剖腹产神经麻醉后运动阻滞消退的时间:一项回顾性队列研究。","authors":"William Shippam, Simon Massey, Kathyrn Clark, Luc Saulnier, Anthony Chau","doi":"10.1111/anae.16400","DOIUrl":null,"url":null,"abstract":"<p>Prolonged motor block regression following neuraxial anaesthesia should prompt careful evaluation for serious postpartum neurological injuries and complications such as vertebral column haematoma. The ability to perform straight leg raise against gravity 4 h after neuraxial anaesthesia has been recommended as a time threshold to trigger review [<span>1</span>]. However, using this time threshold, we observed a large number of our patients required review, resulting in a labour-intensive process that we found difficult to sustain [<span>2</span>]. One possible explanation for the excessive number of triggers may be related to the increased local anaesthetic doses used at our institution, a practice that began during the COVID-19 pandemic and has continued. We hypothesised that the median time to motor block regression after spinal or epidural anaesthesia is > 4 h. To test this, we conducted a retrospective cohort study to characterise the duration of sensory and motor block regression following neuraxial anaesthesia for caesarean delivery (Fig. 1).</p><p>The study was deemed a quality improvement project and research ethics committee approval was not required. Data from 200 patients receiving intrathecal (n = 100, 0.75% hyperbaric bupivacaine with fentanyl 10–15 mcg and morphine 100 mcg) and epidural (n = 100, lidocaine 2% with adrenaline 1:200,000, fentanyl 50–100 mcg and morphine 1.5–2 mg) anaesthesia for elective or emergency caesarean deliveries were retrospectively collected from patient records between December 2021 and February 2022. Sensory and motor evaluations were performed as per our standard institutional protocol. The primary outcome was median time to motor block regression, defined as time of intrathecal injection or epidural top-up, to time of recovery of straight leg raising, analysed using Kaplan–Meier curves with hazard ratio obtained via the Mantel–Haenszel method. Secondary outcomes were median time to motor block regression stratified by intrathecal dose, median time to ambulation and median time to S3 dermatome recovery of sensation to cold.</p><p>Results are presented in Table 1. The maximum time to straight leg raising in outliers was greater with increasing intrathecal dose used, although this study was not powered to examine differences between groups. For sensory block regression, there were significant outliers; four patients in the intrathecal group took 15–21 h for complete motor block regression and four patients in the epidural group took 16–27 h for complete sensory block regression. There were no cases of postpartum neuropathy.</p><p>Using 12.5 mg intrathecal 0.5% hyperbaric bupivacaine, Chapron et al. found the median (IQR [range]) time to complete motor block resolution was 3.7 (3.2–4.2 [1.5–5.0]) h [<span>3</span>]. However, the use of a different dose, concentration and motor block endpoint makes it difficult to directly compare our findings with previous studies. Additionally, there are likely other confounders such as the management of shivering using intravenous dexmedetomidine in some of our patients, that may possibly affect block regression [<span>4</span>]. Unlike intrathecal 0.5% hyperbaric bupivacaine, we found a general lack of block regression data involving 0.75% hyperbaric bupivacaine, and specifically using time to straight leg raising as an endpoint in the obstetric population.</p><p>As > 50% of patients continued to have significant motor block at 4 h following spinal anaesthesia, we extended the time trigger to 6 h. The proportion of patients in our cohort who met the review criteria decreased from 63% to 23% when this threshold was increased. Particularly during periods of high workload, we found excessive reviews with a 100% uneventful outcome have led providers to underestimate the importance of the review process. To raise the specificity for detection of complications, we have since updated our institutional protocol to incorporate an additional criterion: motor and sensory evaluations that have either not improved or worsened over two consecutive assessments. In our experience, this question was frequently asked during assessments to determine if further actions were required. We also found incorporating this criterion at time 0 has significantly decreased the number of reviews triggered while preserving timely review and escalation of care for those with an unusual regression course. Further study on obstetric neuraxial regression times with intrathecal 0.75% hyperbaric bupivacaine and the impact of various time triggers used for neurological monitoring protocols is required.</p>","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":null,"pages":null},"PeriodicalIF":7.5000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16400","citationCount":"0","resultStr":"{\"title\":\"Time to motor block regression after neuraxial anaesthesia for caesarean delivery: a retrospective, cohort study\",\"authors\":\"William Shippam, Simon Massey, Kathyrn Clark, Luc Saulnier, Anthony Chau\",\"doi\":\"10.1111/anae.16400\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Prolonged motor block regression following neuraxial anaesthesia should prompt careful evaluation for serious postpartum neurological injuries and complications such as vertebral column haematoma. The ability to perform straight leg raise against gravity 4 h after neuraxial anaesthesia has been recommended as a time threshold to trigger review [<span>1</span>]. However, using this time threshold, we observed a large number of our patients required review, resulting in a labour-intensive process that we found difficult to sustain [<span>2</span>]. One possible explanation for the excessive number of triggers may be related to the increased local anaesthetic doses used at our institution, a practice that began during the COVID-19 pandemic and has continued. We hypothesised that the median time to motor block regression after spinal or epidural anaesthesia is > 4 h. To test this, we conducted a retrospective cohort study to characterise the duration of sensory and motor block regression following neuraxial anaesthesia for caesarean delivery (Fig. 1).</p><p>The study was deemed a quality improvement project and research ethics committee approval was not required. Data from 200 patients receiving intrathecal (n = 100, 0.75% hyperbaric bupivacaine with fentanyl 10–15 mcg and morphine 100 mcg) and epidural (n = 100, lidocaine 2% with adrenaline 1:200,000, fentanyl 50–100 mcg and morphine 1.5–2 mg) anaesthesia for elective or emergency caesarean deliveries were retrospectively collected from patient records between December 2021 and February 2022. Sensory and motor evaluations were performed as per our standard institutional protocol. The primary outcome was median time to motor block regression, defined as time of intrathecal injection or epidural top-up, to time of recovery of straight leg raising, analysed using Kaplan–Meier curves with hazard ratio obtained via the Mantel–Haenszel method. Secondary outcomes were median time to motor block regression stratified by intrathecal dose, median time to ambulation and median time to S3 dermatome recovery of sensation to cold.</p><p>Results are presented in Table 1. The maximum time to straight leg raising in outliers was greater with increasing intrathecal dose used, although this study was not powered to examine differences between groups. For sensory block regression, there were significant outliers; four patients in the intrathecal group took 15–21 h for complete motor block regression and four patients in the epidural group took 16–27 h for complete sensory block regression. There were no cases of postpartum neuropathy.</p><p>Using 12.5 mg intrathecal 0.5% hyperbaric bupivacaine, Chapron et al. found the median (IQR [range]) time to complete motor block resolution was 3.7 (3.2–4.2 [1.5–5.0]) h [<span>3</span>]. However, the use of a different dose, concentration and motor block endpoint makes it difficult to directly compare our findings with previous studies. Additionally, there are likely other confounders such as the management of shivering using intravenous dexmedetomidine in some of our patients, that may possibly affect block regression [<span>4</span>]. Unlike intrathecal 0.5% hyperbaric bupivacaine, we found a general lack of block regression data involving 0.75% hyperbaric bupivacaine, and specifically using time to straight leg raising as an endpoint in the obstetric population.</p><p>As > 50% of patients continued to have significant motor block at 4 h following spinal anaesthesia, we extended the time trigger to 6 h. The proportion of patients in our cohort who met the review criteria decreased from 63% to 23% when this threshold was increased. Particularly during periods of high workload, we found excessive reviews with a 100% uneventful outcome have led providers to underestimate the importance of the review process. To raise the specificity for detection of complications, we have since updated our institutional protocol to incorporate an additional criterion: motor and sensory evaluations that have either not improved or worsened over two consecutive assessments. In our experience, this question was frequently asked during assessments to determine if further actions were required. We also found incorporating this criterion at time 0 has significantly decreased the number of reviews triggered while preserving timely review and escalation of care for those with an unusual regression course. Further study on obstetric neuraxial regression times with intrathecal 0.75% hyperbaric bupivacaine and the impact of various time triggers used for neurological monitoring protocols is required.</p>\",\"PeriodicalId\":7742,\"journal\":{\"name\":\"Anaesthesia\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16400\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/anae.16400\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anae.16400","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Time to motor block regression after neuraxial anaesthesia for caesarean delivery: a retrospective, cohort study
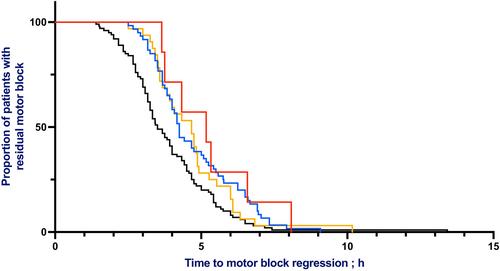
Prolonged motor block regression following neuraxial anaesthesia should prompt careful evaluation for serious postpartum neurological injuries and complications such as vertebral column haematoma. The ability to perform straight leg raise against gravity 4 h after neuraxial anaesthesia has been recommended as a time threshold to trigger review [1]. However, using this time threshold, we observed a large number of our patients required review, resulting in a labour-intensive process that we found difficult to sustain [2]. One possible explanation for the excessive number of triggers may be related to the increased local anaesthetic doses used at our institution, a practice that began during the COVID-19 pandemic and has continued. We hypothesised that the median time to motor block regression after spinal or epidural anaesthesia is > 4 h. To test this, we conducted a retrospective cohort study to characterise the duration of sensory and motor block regression following neuraxial anaesthesia for caesarean delivery (Fig. 1).
The study was deemed a quality improvement project and research ethics committee approval was not required. Data from 200 patients receiving intrathecal (n = 100, 0.75% hyperbaric bupivacaine with fentanyl 10–15 mcg and morphine 100 mcg) and epidural (n = 100, lidocaine 2% with adrenaline 1:200,000, fentanyl 50–100 mcg and morphine 1.5–2 mg) anaesthesia for elective or emergency caesarean deliveries were retrospectively collected from patient records between December 2021 and February 2022. Sensory and motor evaluations were performed as per our standard institutional protocol. The primary outcome was median time to motor block regression, defined as time of intrathecal injection or epidural top-up, to time of recovery of straight leg raising, analysed using Kaplan–Meier curves with hazard ratio obtained via the Mantel–Haenszel method. Secondary outcomes were median time to motor block regression stratified by intrathecal dose, median time to ambulation and median time to S3 dermatome recovery of sensation to cold.
Results are presented in Table 1. The maximum time to straight leg raising in outliers was greater with increasing intrathecal dose used, although this study was not powered to examine differences between groups. For sensory block regression, there were significant outliers; four patients in the intrathecal group took 15–21 h for complete motor block regression and four patients in the epidural group took 16–27 h for complete sensory block regression. There were no cases of postpartum neuropathy.
Using 12.5 mg intrathecal 0.5% hyperbaric bupivacaine, Chapron et al. found the median (IQR [range]) time to complete motor block resolution was 3.7 (3.2–4.2 [1.5–5.0]) h [3]. However, the use of a different dose, concentration and motor block endpoint makes it difficult to directly compare our findings with previous studies. Additionally, there are likely other confounders such as the management of shivering using intravenous dexmedetomidine in some of our patients, that may possibly affect block regression [4]. Unlike intrathecal 0.5% hyperbaric bupivacaine, we found a general lack of block regression data involving 0.75% hyperbaric bupivacaine, and specifically using time to straight leg raising as an endpoint in the obstetric population.
As > 50% of patients continued to have significant motor block at 4 h following spinal anaesthesia, we extended the time trigger to 6 h. The proportion of patients in our cohort who met the review criteria decreased from 63% to 23% when this threshold was increased. Particularly during periods of high workload, we found excessive reviews with a 100% uneventful outcome have led providers to underestimate the importance of the review process. To raise the specificity for detection of complications, we have since updated our institutional protocol to incorporate an additional criterion: motor and sensory evaluations that have either not improved or worsened over two consecutive assessments. In our experience, this question was frequently asked during assessments to determine if further actions were required. We also found incorporating this criterion at time 0 has significantly decreased the number of reviews triggered while preserving timely review and escalation of care for those with an unusual regression course. Further study on obstetric neuraxial regression times with intrathecal 0.75% hyperbaric bupivacaine and the impact of various time triggers used for neurological monitoring protocols is required.
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


