Nadine Kutsch, Sandra Robrecht, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Ilske Oschlies, Matthias Ritgen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Karl-Anton Kreuzer, Stephan Stilgenbauer, Michael Hallek, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst
{"title":"可测量残留疾病时代穿刺骨髓活检的作用--德国 CLL 研究组 (GCLLSG) CLL10 试验的结果。","authors":"Nadine Kutsch, Sandra Robrecht, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Ilske Oschlies, Matthias Ritgen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Karl-Anton Kreuzer, Stephan Stilgenbauer, Michael Hallek, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst","doi":"10.1002/hem3.126","DOIUrl":null,"url":null,"abstract":"<p>The advent of BCL-2 inhibitor-based time-limited therapies has currently replaced chemoimmunotherapy as one standard of care in chronic lymphocytic leukemia (CLL). Despite many differences in efficacy and safety profile, both treatment approaches achieve similarly high rates of undetectable measurable residual disease (U-MRD).<span><sup>1, 2</sup></span> U-MRD has been shown to correlate with progression-free survival (PFS) and even with overall survival (OS) within the MURANO trial,<span><sup>3</sup></span> as well as in the CLL14 trial.<span><sup>4</sup></span> Currently, U-MRD is accepted by the European Medicines Agency (EMA) as intermediate endpoint within clinical trials.<span><sup>5</sup></span></p><p>The iwCLL 2018 response criteria require a bone marrow (BM) aspirate and trephine biopsy for confirmation of complete remission, with immunohistochemistry (IHC) recommended as a tool to differentiate between CLL cells versus benign T- and B-cell infiltrates.<span><sup>6</sup></span> While the prognostic value of measurable residual disease (MRD) in CLL has been extensively studied before,<span><sup>7-11</sup></span> the role of BM assessments by IHC on trephine biopsies has not yet been evaluated. As both BM aspirations and trephine biopsies are collected using an invasive procedure, their added valued remained a matter of debate. Therefore, prognostic value of BM IHC and flow cytometry-based BM MRD assessments is analyzed herein. Moreover, we investigated whether or not sensitive MRD assessments in the peripheral blood (PB) might be able to completely replace the need for BM assessments. Finally, the impact of central versus local pathology investigations are evaluated.</p><p>Patient data were derived from the prospective, randomized CLL10 trial of the GCLLSG, in which chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab (FCR) or bendamustine and rituximab (BR) was administered. BM aspiration and biopsy were performed at final staging 2 months (+28 days) after end of therapy. Central assessment of BM trephine biopsy material for IHC was performed by the hematopathology department in Kiel in conjunction with the prior local pathology. To this end, pathologists aim to identify lymphoid cells with a CLL phenotype in aggregates of lymphoid cells according to the current WHO classification<span><sup>12</sup></span> by superimposing B-cell distribution pattern detected by CD20, CD19, or CD79a with the staining for CD5 and CD23 on separate slides. B-cell markers were stained according to standard protocols on an automated stainer. MRD was assessed in the central laboratory in Kiel by four-color flow cytometry at a threshold of 10<sup>−4</sup> as previously described.<span><sup>13, 14</sup></span></p><p>We compared the impact of MRD and IHC using Kaplan–Meier landmark analyses of PFS and OS from the time point of sample assessment with log-rank tests and Cox proportional hazards regression modeling. Independent prognostic baseline factors for PFS were identified by multivariable analyses using Cox proportional hazards regression modeling with backward and forward selection. All statistical tests were two-sided and <i>p</i> values were descriptive without adjustments for multiple testing. The significance level was set at 0.05.</p><p>Out of 561 patients who were enrolled in the CLL10 trial, 310 patients (55.3%) underwent BM examinations by IHC. Of these, samples from 209 patients (67.4%) were centrally evaluated.</p><p>FCR was administered in 120 (57.4%) of the 209 patients with centrally assessed IHC and 89 patients (42.6%) were treated with BR. For further patient characteristics see Table 1.</p><p>Centrally evaluable samples for BM MRD were available in 168 of 209 patients (80.4%). Out of these 168 samples, seven samples (4.2%) tested IHC positive (+) with BM U-MRD, 77 samples (45.8%) tested IHC negative (−) with BM U-MRD, 53 samples (31.5%) were IHC+ with BM detectable MRD (D-MRD), and 31 (18.5%) had discordantly IHC−/BM D-MRD. Patients with BM U-MRD had an estimated 3-year PFS rate from landmark of 100% if simultaneously IHC+ and an estimated 3-year PFS rate from landmark of 92.9% if IHC− (log-rank <i>p</i> = 0.202). Thus, IHC does not seem to contribute to identification of low-risk disease once BM U-MRD is known. In BM D-MRD patients, simultaneous IHC+ showed an estimated 3-year PFS rate from landmark of 31.7%, compared to concordant IHC− with an estimated 3-year PFS rate from landmark of 59.8% (HR = 2.062, 95% confidence interval [CI]: 1.155–3.683, <i>p</i> = 0.014). Detecting CLL by IHC in BM D-MRD patients might contribute to identify patients suffering from persistent high-level disease with a poor PFS (Figure 1A). However, very high-risk disease might be identified in the BM and PB with similar accuracy using an additional cut-off at an MRD threshold of 10<sup>−2</sup>.<span><sup>7</sup></span> The estimated 3-year OS-rate from landmark was 100.0% for patients with IHC+/BM U-MRD, whereas patients with IHC−/BM U-MRD had an estimated 3-year OS-rate from landmark of 97.3% (log-rank <i>p</i> = 0.537). For patients with IHC+/BM D-MRD, the estimated 3-year OS-rate from landmark was 94.1% versus 100.0% in patients with IHC−/BM D-MRD (HR = 0.368; 95% CI: 0.108–1.258, <i>p</i> = 0.111) (Figure 1A).</p><p>Analyzing patients with U-MRD in the PB, the estimated 3-year PFS rate was 51.3% for 33 IHC+ patients, compared to 101 patients with IHC− who had an estimated 3-year PFS rate of 83.3% (HR = 2.646, 95% CI: 1.488–4.705, <i>p</i> < 0.001). For 29 patients with IHC+ and PB D-MRD, the estimated 3-year PFS rate was 30.7% compared to 55.6% in nine patients with IHC−/PB D-MRD (HR = 2.035, 95% CI: 0.772–5.368, <i>p</i> = 0.151) (Figure 1B). The estimated 3-year OS-rate was 100.0% for patients with IHC+/PB U-MRD and 98.0% for patients with IHC−/PB U-MRD (HR = 0.668, 95% CI: 0.146–3.050, <i>p</i> = 0.602). Patients with IHC+/PB D-MRD had an estimated 3-year OS-rate from landmark of 89.1% and patients with IHC−/PB D-MRD of 100.0% (HR = 0.364, 95% CI: 0.073–1.807, <i>p</i> = 0.216) (Figure 1B).</p><p>Next, we investigated whether PB MRD assessments could completely replace both BM investigations, thus obviating the need for this invasive procedure. In univariable analysis, treatment arm, BM infiltration by IHC and MRD in PB and BM, as well as del(11q) status, IGHV mutational status, and serum thymidine kinase at baseline, were identified as prognostic factors for PFS. When considering all these variables in the multivariable analysis, flow MRD in the BM as well as IGHV mutational status were suggested as independent prognostic factors for PFS. We conclude that for better prognostication a flow-based MRD assessment of a BM aspirate remains necessary. Once BM MRD is known, there seems to be no added value of a trephine biopsy, which might be omitted. When excluding MRD from multivariable analysis, treatment arm, IGHV mutational status, and BM infiltration by IHC were identified as independent prognostic factors. Thus, if no MRD assessments are available, a BM examination seems to contribute to prognostication. Multivariable analysis for OS was not performed as BM infiltration by IHC was not significantly associated with landmark OS in univariable analyses.</p><p>Within the total population of 310 patients with both locally and centrally assessed IHC, we found that IHC+, evaluated as a single parameter, was associated with shorter PFS as the estimated 3-year PFS rate from landmark was 39.3% versus 77.5% in IHC− (HR = 2.671, 95% CI: 1.942–3.674, <i>p</i> < 0.001). We thereafter evaluated the prognostic value of IHC when assessed in local versus central laboratories. Interestingly, IHC− patients with IHC evaluated in a local laboratory (estimated 3-year PFS-rate 68.0%) carried a poorer prognosis compared to patients with IHC tested in the central laboratory (estimated 3-year PFS-rate 82.2%, HR = 1.756, 95% CI: 1.108–2.782, <i>p</i> = 0.017). This finding suggests a better specificity of the reference laboratory for IHC− results. The estimated 3-year PFS-rate from landmark for patients with IHC+ was 33.3% for local versus 42.5% for the central laboratory (HR = 1.160, 95% CI: 0.733–1.834; <i>p</i> = 0.527) (Figure 1C). The difference between local and central laboratory in IHC− samples might be explained by the fact that there was no common standard when evaluating the local samples. Thus, whenever a trephine biopsy is taken, an assessment in a reference pathology laboratory is advisable.</p><p>When investigating OS from landmark time point of sample assessment according to BM infiltration by IHC and local versus central laboratory, no significant differences were detected. This might be explained by effective subsequent treatments. The estimated 3-year OS-rate from landmark for patients with IHC− was 93.5% if assessed by local laboratory and 98.5% by central laboratory (HR = 1.983, 95% CI: 0.943–4.170, <i>p</i> = 0.071). The estimated 3-year OS-rate from landmark for patients with IHC+ was 82.6% for local laboratory and 93.1% for central laboratory (HR = 2.114, 95% CI: 0.793–5.639, <i>p</i> = 0.135) (Figure 1C).</p><p>In summary, we could confirm that MRD seems to be a valid prognostic parameter for PFS for time-limited therapies, although these data comprise only chemoimmunotherapies and should be reevaluated for targeted agents if data on both, MRD and IHC, are available. This is consistent with a pooled analysis of phase 3 trials based on chemoimmunotherapy combinations (CLL8, CLL10, CLL11), which has also shown a significant relationship between MRD in the PB and PFS.<span><sup>11</sup></span> Within this patient population of the CLL10 trial, no statistically relevant difference in OS could be shown. IHC was confirmed as an independent prognostic marker in multivariable analysis for PFS when flow cytometry-based MRD was excluded.</p><p>Although both methods, flow MRD as well as IHC, add valuable information on depth of response, the results of the multivariable analyses indicate that flow MRD in BM provides the prognostic information needed and patients may be spared an additional biopsy. If a biopsy is performed, we recommend to evaluate the histology centrally to improve the prognostic value of the assessment.</p><p>Nadine Kutsch, Sandra Robrecht, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst conceived and designed the analysis. Nadine Kutsch, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Michael Hallek, Barbara Eichhorst collected the data. Ilske Oschlies, Matthias Ritgen, Karl-Anton Kreuzer, Stephan Stilgenbauer, Sebastian Böttcher, Wolfram Klapper contributed data or analysis tools. Sandra Robrecht performed the statistical analysis. Nadine Kutsch wrote the first draft of the paper. All authors contributed to manuscript revision, read, and approved the submitted version.</p><p>Nadine Kutsch: Honoraria: AbbVie, AstraZeneca, BMS, Kite/Gilead; Research support: AstraZeneca, Gilead. travel grants: AbbVie, AstraZeneca, Beigene, Celgene, Janssen. Sandra Robrecht: Honoraria: AstraZeneca. Anna Fink: Research funding: AstraZeneca and Celgene, Travel grants: AbbVie. Elisabeth Lange: no COIs. Rudolf Weide: Personal fees from AstraZeneca, BeiGene, Biotest, CSL Behring, Daiichi Sankyo, Eisai, Gilead, Hexal, Incyte, Medac, Menarini-Stemline, Pierre Fabre, Roche, SeaGen, Sobi, and Takeda. Our institution has received research funding from Amgen, Biotest, Celgene, CSL Behring, Daiichi Sankyo, Eisai, GSK, Hexal, Lilly, Medac, Mundipharma, Octapharma, Sobi, and Takeda. Michael G. Kiehl: no COIs. Martin Sökler: no COIs. Rudolf Schlag: no COIs. Ursula Vehling-Kaiser: no COIs. Georg Köchling: no COIs. Christoph Plöger: no COIs. Michael Gregor: no COIs. Torben Plesner: advisory board: Celgene/BMS. Michael R. Clausen: no COIs. Ilske Oschlies: no COIs. Matthias Ritgen: grants from F. Hoffman-La Roche; and personal fees from F. Hoffmann-La Roche and AbbVie. Marco Herling: no COIs. Kirsten Fischer: Advisory Board: AbbVie, Roche, AstaZeneca, Honoraria: Roche, AstraZeneca, Travel Support: Roche. Hartmut Döhner: Advisory role with honoraria for AbbVie, AstraZeneca, Gilead, Janssen, Jazz, Pfizer, Servier, Stemline, Syndax; clinical research funding (to institution) from AbbVie, Astellas, Bristol Myers Squibb, Celgene, Jazz Pharmaceuticals, Kronos Bio, Servier. Clemens-Martin Wendtner: Research grants, advisory boards and travel grants by Hoffmann-La Roche, Janssen-Cilag, AstraZeneca, AbbVie, BeiGene and GSK. Karl-Anton Kreuzer: consultant or advisory board member, honoraria and research support by AbbVie, Amgen, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Stephan Stilgenbauer: Advisory board, honoraria, research support, travel support, speaker fees, trial participation: AbbVie, Amgen, AstraZeneca, BeiGene, BMS, Celgene, Gilead, GSK, Hoffmann-La Roche, Janssen, Lilly, Novartis, Sunesis. Michael Hallek: Consultant or advisory board member, honoraria, and research support by AbbVie, Amgen, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Sebastian Böttcher: research funding from Janssen and AbbVie; and honoraria from Roche, Janssen, AbbVie, Novartis, Becton Dickinson, AstraZeneca, and Sanofi. Wolfram Klapper: Research grants from Roche, Amgen, Janssen, InCyte Regeneraon, Takeda and advisory role (Roche) paid to my institution. All without relevance for the current manuscript. Barbara Eichhorst: Consultant or advisory board member, research support or travel support by AbbVie, AstraZeneca, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag.</p><p>The authors declare no sources of funding.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11267170/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of trephine bone marrow biopsies in the era of measurable residual disease—Results from the CLL10 trial of the German CLL Study Group (GCLLSG)\",\"authors\":\"Nadine Kutsch, Sandra Robrecht, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Ilske Oschlies, Matthias Ritgen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Karl-Anton Kreuzer, Stephan Stilgenbauer, Michael Hallek, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst\",\"doi\":\"10.1002/hem3.126\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The advent of BCL-2 inhibitor-based time-limited therapies has currently replaced chemoimmunotherapy as one standard of care in chronic lymphocytic leukemia (CLL). Despite many differences in efficacy and safety profile, both treatment approaches achieve similarly high rates of undetectable measurable residual disease (U-MRD).<span><sup>1, 2</sup></span> U-MRD has been shown to correlate with progression-free survival (PFS) and even with overall survival (OS) within the MURANO trial,<span><sup>3</sup></span> as well as in the CLL14 trial.<span><sup>4</sup></span> Currently, U-MRD is accepted by the European Medicines Agency (EMA) as intermediate endpoint within clinical trials.<span><sup>5</sup></span></p><p>The iwCLL 2018 response criteria require a bone marrow (BM) aspirate and trephine biopsy for confirmation of complete remission, with immunohistochemistry (IHC) recommended as a tool to differentiate between CLL cells versus benign T- and B-cell infiltrates.<span><sup>6</sup></span> While the prognostic value of measurable residual disease (MRD) in CLL has been extensively studied before,<span><sup>7-11</sup></span> the role of BM assessments by IHC on trephine biopsies has not yet been evaluated. As both BM aspirations and trephine biopsies are collected using an invasive procedure, their added valued remained a matter of debate. Therefore, prognostic value of BM IHC and flow cytometry-based BM MRD assessments is analyzed herein. Moreover, we investigated whether or not sensitive MRD assessments in the peripheral blood (PB) might be able to completely replace the need for BM assessments. Finally, the impact of central versus local pathology investigations are evaluated.</p><p>Patient data were derived from the prospective, randomized CLL10 trial of the GCLLSG, in which chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab (FCR) or bendamustine and rituximab (BR) was administered. BM aspiration and biopsy were performed at final staging 2 months (+28 days) after end of therapy. Central assessment of BM trephine biopsy material for IHC was performed by the hematopathology department in Kiel in conjunction with the prior local pathology. To this end, pathologists aim to identify lymphoid cells with a CLL phenotype in aggregates of lymphoid cells according to the current WHO classification<span><sup>12</sup></span> by superimposing B-cell distribution pattern detected by CD20, CD19, or CD79a with the staining for CD5 and CD23 on separate slides. B-cell markers were stained according to standard protocols on an automated stainer. MRD was assessed in the central laboratory in Kiel by four-color flow cytometry at a threshold of 10<sup>−4</sup> as previously described.<span><sup>13, 14</sup></span></p><p>We compared the impact of MRD and IHC using Kaplan–Meier landmark analyses of PFS and OS from the time point of sample assessment with log-rank tests and Cox proportional hazards regression modeling. Independent prognostic baseline factors for PFS were identified by multivariable analyses using Cox proportional hazards regression modeling with backward and forward selection. All statistical tests were two-sided and <i>p</i> values were descriptive without adjustments for multiple testing. The significance level was set at 0.05.</p><p>Out of 561 patients who were enrolled in the CLL10 trial, 310 patients (55.3%) underwent BM examinations by IHC. Of these, samples from 209 patients (67.4%) were centrally evaluated.</p><p>FCR was administered in 120 (57.4%) of the 209 patients with centrally assessed IHC and 89 patients (42.6%) were treated with BR. For further patient characteristics see Table 1.</p><p>Centrally evaluable samples for BM MRD were available in 168 of 209 patients (80.4%). Out of these 168 samples, seven samples (4.2%) tested IHC positive (+) with BM U-MRD, 77 samples (45.8%) tested IHC negative (−) with BM U-MRD, 53 samples (31.5%) were IHC+ with BM detectable MRD (D-MRD), and 31 (18.5%) had discordantly IHC−/BM D-MRD. Patients with BM U-MRD had an estimated 3-year PFS rate from landmark of 100% if simultaneously IHC+ and an estimated 3-year PFS rate from landmark of 92.9% if IHC− (log-rank <i>p</i> = 0.202). Thus, IHC does not seem to contribute to identification of low-risk disease once BM U-MRD is known. In BM D-MRD patients, simultaneous IHC+ showed an estimated 3-year PFS rate from landmark of 31.7%, compared to concordant IHC− with an estimated 3-year PFS rate from landmark of 59.8% (HR = 2.062, 95% confidence interval [CI]: 1.155–3.683, <i>p</i> = 0.014). Detecting CLL by IHC in BM D-MRD patients might contribute to identify patients suffering from persistent high-level disease with a poor PFS (Figure 1A). However, very high-risk disease might be identified in the BM and PB with similar accuracy using an additional cut-off at an MRD threshold of 10<sup>−2</sup>.<span><sup>7</sup></span> The estimated 3-year OS-rate from landmark was 100.0% for patients with IHC+/BM U-MRD, whereas patients with IHC−/BM U-MRD had an estimated 3-year OS-rate from landmark of 97.3% (log-rank <i>p</i> = 0.537). For patients with IHC+/BM D-MRD, the estimated 3-year OS-rate from landmark was 94.1% versus 100.0% in patients with IHC−/BM D-MRD (HR = 0.368; 95% CI: 0.108–1.258, <i>p</i> = 0.111) (Figure 1A).</p><p>Analyzing patients with U-MRD in the PB, the estimated 3-year PFS rate was 51.3% for 33 IHC+ patients, compared to 101 patients with IHC− who had an estimated 3-year PFS rate of 83.3% (HR = 2.646, 95% CI: 1.488–4.705, <i>p</i> < 0.001). For 29 patients with IHC+ and PB D-MRD, the estimated 3-year PFS rate was 30.7% compared to 55.6% in nine patients with IHC−/PB D-MRD (HR = 2.035, 95% CI: 0.772–5.368, <i>p</i> = 0.151) (Figure 1B). The estimated 3-year OS-rate was 100.0% for patients with IHC+/PB U-MRD and 98.0% for patients with IHC−/PB U-MRD (HR = 0.668, 95% CI: 0.146–3.050, <i>p</i> = 0.602). Patients with IHC+/PB D-MRD had an estimated 3-year OS-rate from landmark of 89.1% and patients with IHC−/PB D-MRD of 100.0% (HR = 0.364, 95% CI: 0.073–1.807, <i>p</i> = 0.216) (Figure 1B).</p><p>Next, we investigated whether PB MRD assessments could completely replace both BM investigations, thus obviating the need for this invasive procedure. In univariable analysis, treatment arm, BM infiltration by IHC and MRD in PB and BM, as well as del(11q) status, IGHV mutational status, and serum thymidine kinase at baseline, were identified as prognostic factors for PFS. When considering all these variables in the multivariable analysis, flow MRD in the BM as well as IGHV mutational status were suggested as independent prognostic factors for PFS. We conclude that for better prognostication a flow-based MRD assessment of a BM aspirate remains necessary. Once BM MRD is known, there seems to be no added value of a trephine biopsy, which might be omitted. When excluding MRD from multivariable analysis, treatment arm, IGHV mutational status, and BM infiltration by IHC were identified as independent prognostic factors. Thus, if no MRD assessments are available, a BM examination seems to contribute to prognostication. Multivariable analysis for OS was not performed as BM infiltration by IHC was not significantly associated with landmark OS in univariable analyses.</p><p>Within the total population of 310 patients with both locally and centrally assessed IHC, we found that IHC+, evaluated as a single parameter, was associated with shorter PFS as the estimated 3-year PFS rate from landmark was 39.3% versus 77.5% in IHC− (HR = 2.671, 95% CI: 1.942–3.674, <i>p</i> < 0.001). We thereafter evaluated the prognostic value of IHC when assessed in local versus central laboratories. Interestingly, IHC− patients with IHC evaluated in a local laboratory (estimated 3-year PFS-rate 68.0%) carried a poorer prognosis compared to patients with IHC tested in the central laboratory (estimated 3-year PFS-rate 82.2%, HR = 1.756, 95% CI: 1.108–2.782, <i>p</i> = 0.017). This finding suggests a better specificity of the reference laboratory for IHC− results. The estimated 3-year PFS-rate from landmark for patients with IHC+ was 33.3% for local versus 42.5% for the central laboratory (HR = 1.160, 95% CI: 0.733–1.834; <i>p</i> = 0.527) (Figure 1C). The difference between local and central laboratory in IHC− samples might be explained by the fact that there was no common standard when evaluating the local samples. Thus, whenever a trephine biopsy is taken, an assessment in a reference pathology laboratory is advisable.</p><p>When investigating OS from landmark time point of sample assessment according to BM infiltration by IHC and local versus central laboratory, no significant differences were detected. This might be explained by effective subsequent treatments. The estimated 3-year OS-rate from landmark for patients with IHC− was 93.5% if assessed by local laboratory and 98.5% by central laboratory (HR = 1.983, 95% CI: 0.943–4.170, <i>p</i> = 0.071). The estimated 3-year OS-rate from landmark for patients with IHC+ was 82.6% for local laboratory and 93.1% for central laboratory (HR = 2.114, 95% CI: 0.793–5.639, <i>p</i> = 0.135) (Figure 1C).</p><p>In summary, we could confirm that MRD seems to be a valid prognostic parameter for PFS for time-limited therapies, although these data comprise only chemoimmunotherapies and should be reevaluated for targeted agents if data on both, MRD and IHC, are available. This is consistent with a pooled analysis of phase 3 trials based on chemoimmunotherapy combinations (CLL8, CLL10, CLL11), which has also shown a significant relationship between MRD in the PB and PFS.<span><sup>11</sup></span> Within this patient population of the CLL10 trial, no statistically relevant difference in OS could be shown. IHC was confirmed as an independent prognostic marker in multivariable analysis for PFS when flow cytometry-based MRD was excluded.</p><p>Although both methods, flow MRD as well as IHC, add valuable information on depth of response, the results of the multivariable analyses indicate that flow MRD in BM provides the prognostic information needed and patients may be spared an additional biopsy. If a biopsy is performed, we recommend to evaluate the histology centrally to improve the prognostic value of the assessment.</p><p>Nadine Kutsch, Sandra Robrecht, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst conceived and designed the analysis. Nadine Kutsch, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Michael Hallek, Barbara Eichhorst collected the data. Ilske Oschlies, Matthias Ritgen, Karl-Anton Kreuzer, Stephan Stilgenbauer, Sebastian Böttcher, Wolfram Klapper contributed data or analysis tools. Sandra Robrecht performed the statistical analysis. Nadine Kutsch wrote the first draft of the paper. All authors contributed to manuscript revision, read, and approved the submitted version.</p><p>Nadine Kutsch: Honoraria: AbbVie, AstraZeneca, BMS, Kite/Gilead; Research support: AstraZeneca, Gilead. travel grants: AbbVie, AstraZeneca, Beigene, Celgene, Janssen. Sandra Robrecht: Honoraria: AstraZeneca. Anna Fink: Research funding: AstraZeneca and Celgene, Travel grants: AbbVie. Elisabeth Lange: no COIs. Rudolf Weide: Personal fees from AstraZeneca, BeiGene, Biotest, CSL Behring, Daiichi Sankyo, Eisai, Gilead, Hexal, Incyte, Medac, Menarini-Stemline, Pierre Fabre, Roche, SeaGen, Sobi, and Takeda. Our institution has received research funding from Amgen, Biotest, Celgene, CSL Behring, Daiichi Sankyo, Eisai, GSK, Hexal, Lilly, Medac, Mundipharma, Octapharma, Sobi, and Takeda. Michael G. Kiehl: no COIs. Martin Sökler: no COIs. Rudolf Schlag: no COIs. Ursula Vehling-Kaiser: no COIs. Georg Köchling: no COIs. Christoph Plöger: no COIs. Michael Gregor: no COIs. Torben Plesner: advisory board: Celgene/BMS. Michael R. Clausen: no COIs. Ilske Oschlies: no COIs. Matthias Ritgen: grants from F. Hoffman-La Roche; and personal fees from F. Hoffmann-La Roche and AbbVie. Marco Herling: no COIs. Kirsten Fischer: Advisory Board: AbbVie, Roche, AstaZeneca, Honoraria: Roche, AstraZeneca, Travel Support: Roche. Hartmut Döhner: Advisory role with honoraria for AbbVie, AstraZeneca, Gilead, Janssen, Jazz, Pfizer, Servier, Stemline, Syndax; clinical research funding (to institution) from AbbVie, Astellas, Bristol Myers Squibb, Celgene, Jazz Pharmaceuticals, Kronos Bio, Servier. Clemens-Martin Wendtner: Research grants, advisory boards and travel grants by Hoffmann-La Roche, Janssen-Cilag, AstraZeneca, AbbVie, BeiGene and GSK. Karl-Anton Kreuzer: consultant or advisory board member, honoraria and research support by AbbVie, Amgen, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Stephan Stilgenbauer: Advisory board, honoraria, research support, travel support, speaker fees, trial participation: AbbVie, Amgen, AstraZeneca, BeiGene, BMS, Celgene, Gilead, GSK, Hoffmann-La Roche, Janssen, Lilly, Novartis, Sunesis. Michael Hallek: Consultant or advisory board member, honoraria, and research support by AbbVie, Amgen, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Sebastian Böttcher: research funding from Janssen and AbbVie; and honoraria from Roche, Janssen, AbbVie, Novartis, Becton Dickinson, AstraZeneca, and Sanofi. Wolfram Klapper: Research grants from Roche, Amgen, Janssen, InCyte Regeneraon, Takeda and advisory role (Roche) paid to my institution. All without relevance for the current manuscript. Barbara Eichhorst: Consultant or advisory board member, research support or travel support by AbbVie, AstraZeneca, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag.</p><p>The authors declare no sources of funding.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 7\",\"pages\":\"\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2024-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11267170/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.126\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.126","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
The role of trephine bone marrow biopsies in the era of measurable residual disease—Results from the CLL10 trial of the German CLL Study Group (GCLLSG)
The advent of BCL-2 inhibitor-based time-limited therapies has currently replaced chemoimmunotherapy as one standard of care in chronic lymphocytic leukemia (CLL). Despite many differences in efficacy and safety profile, both treatment approaches achieve similarly high rates of undetectable measurable residual disease (U-MRD).1, 2 U-MRD has been shown to correlate with progression-free survival (PFS) and even with overall survival (OS) within the MURANO trial,3 as well as in the CLL14 trial.4 Currently, U-MRD is accepted by the European Medicines Agency (EMA) as intermediate endpoint within clinical trials.5
The iwCLL 2018 response criteria require a bone marrow (BM) aspirate and trephine biopsy for confirmation of complete remission, with immunohistochemistry (IHC) recommended as a tool to differentiate between CLL cells versus benign T- and B-cell infiltrates.6 While the prognostic value of measurable residual disease (MRD) in CLL has been extensively studied before,7-11 the role of BM assessments by IHC on trephine biopsies has not yet been evaluated. As both BM aspirations and trephine biopsies are collected using an invasive procedure, their added valued remained a matter of debate. Therefore, prognostic value of BM IHC and flow cytometry-based BM MRD assessments is analyzed herein. Moreover, we investigated whether or not sensitive MRD assessments in the peripheral blood (PB) might be able to completely replace the need for BM assessments. Finally, the impact of central versus local pathology investigations are evaluated.
Patient data were derived from the prospective, randomized CLL10 trial of the GCLLSG, in which chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab (FCR) or bendamustine and rituximab (BR) was administered. BM aspiration and biopsy were performed at final staging 2 months (+28 days) after end of therapy. Central assessment of BM trephine biopsy material for IHC was performed by the hematopathology department in Kiel in conjunction with the prior local pathology. To this end, pathologists aim to identify lymphoid cells with a CLL phenotype in aggregates of lymphoid cells according to the current WHO classification12 by superimposing B-cell distribution pattern detected by CD20, CD19, or CD79a with the staining for CD5 and CD23 on separate slides. B-cell markers were stained according to standard protocols on an automated stainer. MRD was assessed in the central laboratory in Kiel by four-color flow cytometry at a threshold of 10−4 as previously described.13, 14
We compared the impact of MRD and IHC using Kaplan–Meier landmark analyses of PFS and OS from the time point of sample assessment with log-rank tests and Cox proportional hazards regression modeling. Independent prognostic baseline factors for PFS were identified by multivariable analyses using Cox proportional hazards regression modeling with backward and forward selection. All statistical tests were two-sided and p values were descriptive without adjustments for multiple testing. The significance level was set at 0.05.
Out of 561 patients who were enrolled in the CLL10 trial, 310 patients (55.3%) underwent BM examinations by IHC. Of these, samples from 209 patients (67.4%) were centrally evaluated.
FCR was administered in 120 (57.4%) of the 209 patients with centrally assessed IHC and 89 patients (42.6%) were treated with BR. For further patient characteristics see Table 1.
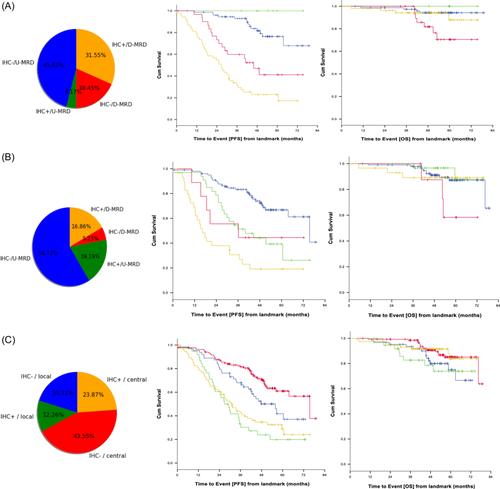
Centrally evaluable samples for BM MRD were available in 168 of 209 patients (80.4%). Out of these 168 samples, seven samples (4.2%) tested IHC positive (+) with BM U-MRD, 77 samples (45.8%) tested IHC negative (−) with BM U-MRD, 53 samples (31.5%) were IHC+ with BM detectable MRD (D-MRD), and 31 (18.5%) had discordantly IHC−/BM D-MRD. Patients with BM U-MRD had an estimated 3-year PFS rate from landmark of 100% if simultaneously IHC+ and an estimated 3-year PFS rate from landmark of 92.9% if IHC− (log-rank p = 0.202). Thus, IHC does not seem to contribute to identification of low-risk disease once BM U-MRD is known. In BM D-MRD patients, simultaneous IHC+ showed an estimated 3-year PFS rate from landmark of 31.7%, compared to concordant IHC− with an estimated 3-year PFS rate from landmark of 59.8% (HR = 2.062, 95% confidence interval [CI]: 1.155–3.683, p = 0.014). Detecting CLL by IHC in BM D-MRD patients might contribute to identify patients suffering from persistent high-level disease with a poor PFS (Figure 1A). However, very high-risk disease might be identified in the BM and PB with similar accuracy using an additional cut-off at an MRD threshold of 10−2.7 The estimated 3-year OS-rate from landmark was 100.0% for patients with IHC+/BM U-MRD, whereas patients with IHC−/BM U-MRD had an estimated 3-year OS-rate from landmark of 97.3% (log-rank p = 0.537). For patients with IHC+/BM D-MRD, the estimated 3-year OS-rate from landmark was 94.1% versus 100.0% in patients with IHC−/BM D-MRD (HR = 0.368; 95% CI: 0.108–1.258, p = 0.111) (Figure 1A).
Analyzing patients with U-MRD in the PB, the estimated 3-year PFS rate was 51.3% for 33 IHC+ patients, compared to 101 patients with IHC− who had an estimated 3-year PFS rate of 83.3% (HR = 2.646, 95% CI: 1.488–4.705, p < 0.001). For 29 patients with IHC+ and PB D-MRD, the estimated 3-year PFS rate was 30.7% compared to 55.6% in nine patients with IHC−/PB D-MRD (HR = 2.035, 95% CI: 0.772–5.368, p = 0.151) (Figure 1B). The estimated 3-year OS-rate was 100.0% for patients with IHC+/PB U-MRD and 98.0% for patients with IHC−/PB U-MRD (HR = 0.668, 95% CI: 0.146–3.050, p = 0.602). Patients with IHC+/PB D-MRD had an estimated 3-year OS-rate from landmark of 89.1% and patients with IHC−/PB D-MRD of 100.0% (HR = 0.364, 95% CI: 0.073–1.807, p = 0.216) (Figure 1B).
Next, we investigated whether PB MRD assessments could completely replace both BM investigations, thus obviating the need for this invasive procedure. In univariable analysis, treatment arm, BM infiltration by IHC and MRD in PB and BM, as well as del(11q) status, IGHV mutational status, and serum thymidine kinase at baseline, were identified as prognostic factors for PFS. When considering all these variables in the multivariable analysis, flow MRD in the BM as well as IGHV mutational status were suggested as independent prognostic factors for PFS. We conclude that for better prognostication a flow-based MRD assessment of a BM aspirate remains necessary. Once BM MRD is known, there seems to be no added value of a trephine biopsy, which might be omitted. When excluding MRD from multivariable analysis, treatment arm, IGHV mutational status, and BM infiltration by IHC were identified as independent prognostic factors. Thus, if no MRD assessments are available, a BM examination seems to contribute to prognostication. Multivariable analysis for OS was not performed as BM infiltration by IHC was not significantly associated with landmark OS in univariable analyses.
Within the total population of 310 patients with both locally and centrally assessed IHC, we found that IHC+, evaluated as a single parameter, was associated with shorter PFS as the estimated 3-year PFS rate from landmark was 39.3% versus 77.5% in IHC− (HR = 2.671, 95% CI: 1.942–3.674, p < 0.001). We thereafter evaluated the prognostic value of IHC when assessed in local versus central laboratories. Interestingly, IHC− patients with IHC evaluated in a local laboratory (estimated 3-year PFS-rate 68.0%) carried a poorer prognosis compared to patients with IHC tested in the central laboratory (estimated 3-year PFS-rate 82.2%, HR = 1.756, 95% CI: 1.108–2.782, p = 0.017). This finding suggests a better specificity of the reference laboratory for IHC− results. The estimated 3-year PFS-rate from landmark for patients with IHC+ was 33.3% for local versus 42.5% for the central laboratory (HR = 1.160, 95% CI: 0.733–1.834; p = 0.527) (Figure 1C). The difference between local and central laboratory in IHC− samples might be explained by the fact that there was no common standard when evaluating the local samples. Thus, whenever a trephine biopsy is taken, an assessment in a reference pathology laboratory is advisable.
When investigating OS from landmark time point of sample assessment according to BM infiltration by IHC and local versus central laboratory, no significant differences were detected. This might be explained by effective subsequent treatments. The estimated 3-year OS-rate from landmark for patients with IHC− was 93.5% if assessed by local laboratory and 98.5% by central laboratory (HR = 1.983, 95% CI: 0.943–4.170, p = 0.071). The estimated 3-year OS-rate from landmark for patients with IHC+ was 82.6% for local laboratory and 93.1% for central laboratory (HR = 2.114, 95% CI: 0.793–5.639, p = 0.135) (Figure 1C).
In summary, we could confirm that MRD seems to be a valid prognostic parameter for PFS for time-limited therapies, although these data comprise only chemoimmunotherapies and should be reevaluated for targeted agents if data on both, MRD and IHC, are available. This is consistent with a pooled analysis of phase 3 trials based on chemoimmunotherapy combinations (CLL8, CLL10, CLL11), which has also shown a significant relationship between MRD in the PB and PFS.11 Within this patient population of the CLL10 trial, no statistically relevant difference in OS could be shown. IHC was confirmed as an independent prognostic marker in multivariable analysis for PFS when flow cytometry-based MRD was excluded.
Although both methods, flow MRD as well as IHC, add valuable information on depth of response, the results of the multivariable analyses indicate that flow MRD in BM provides the prognostic information needed and patients may be spared an additional biopsy. If a biopsy is performed, we recommend to evaluate the histology centrally to improve the prognostic value of the assessment.
Nadine Kutsch, Sandra Robrecht, Sebastian Böttcher, Wolfram Klapper, Barbara Eichhorst conceived and designed the analysis. Nadine Kutsch, Anna Fink, Elisabeth Lange, Rudolf Weide, Michael G. Kiehl, Martin Sökler, Rudolf Schlag, Ursula Vehling-Kaiser, Georg Köchling, Christoph Plöger, Michael Gregor, Torben Plesner, Michael R. Clausen, Marco Herling, Kirsten Fischer, Hartmut Döhner, Clemens-Martin Wendtner, Michael Hallek, Barbara Eichhorst collected the data. Ilske Oschlies, Matthias Ritgen, Karl-Anton Kreuzer, Stephan Stilgenbauer, Sebastian Böttcher, Wolfram Klapper contributed data or analysis tools. Sandra Robrecht performed the statistical analysis. Nadine Kutsch wrote the first draft of the paper. All authors contributed to manuscript revision, read, and approved the submitted version.
Nadine Kutsch: Honoraria: AbbVie, AstraZeneca, BMS, Kite/Gilead; Research support: AstraZeneca, Gilead. travel grants: AbbVie, AstraZeneca, Beigene, Celgene, Janssen. Sandra Robrecht: Honoraria: AstraZeneca. Anna Fink: Research funding: AstraZeneca and Celgene, Travel grants: AbbVie. Elisabeth Lange: no COIs. Rudolf Weide: Personal fees from AstraZeneca, BeiGene, Biotest, CSL Behring, Daiichi Sankyo, Eisai, Gilead, Hexal, Incyte, Medac, Menarini-Stemline, Pierre Fabre, Roche, SeaGen, Sobi, and Takeda. Our institution has received research funding from Amgen, Biotest, Celgene, CSL Behring, Daiichi Sankyo, Eisai, GSK, Hexal, Lilly, Medac, Mundipharma, Octapharma, Sobi, and Takeda. Michael G. Kiehl: no COIs. Martin Sökler: no COIs. Rudolf Schlag: no COIs. Ursula Vehling-Kaiser: no COIs. Georg Köchling: no COIs. Christoph Plöger: no COIs. Michael Gregor: no COIs. Torben Plesner: advisory board: Celgene/BMS. Michael R. Clausen: no COIs. Ilske Oschlies: no COIs. Matthias Ritgen: grants from F. Hoffman-La Roche; and personal fees from F. Hoffmann-La Roche and AbbVie. Marco Herling: no COIs. Kirsten Fischer: Advisory Board: AbbVie, Roche, AstaZeneca, Honoraria: Roche, AstraZeneca, Travel Support: Roche. Hartmut Döhner: Advisory role with honoraria for AbbVie, AstraZeneca, Gilead, Janssen, Jazz, Pfizer, Servier, Stemline, Syndax; clinical research funding (to institution) from AbbVie, Astellas, Bristol Myers Squibb, Celgene, Jazz Pharmaceuticals, Kronos Bio, Servier. Clemens-Martin Wendtner: Research grants, advisory boards and travel grants by Hoffmann-La Roche, Janssen-Cilag, AstraZeneca, AbbVie, BeiGene and GSK. Karl-Anton Kreuzer: consultant or advisory board member, honoraria and research support by AbbVie, Amgen, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Stephan Stilgenbauer: Advisory board, honoraria, research support, travel support, speaker fees, trial participation: AbbVie, Amgen, AstraZeneca, BeiGene, BMS, Celgene, Gilead, GSK, Hoffmann-La Roche, Janssen, Lilly, Novartis, Sunesis. Michael Hallek: Consultant or advisory board member, honoraria, and research support by AbbVie, Amgen, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag and Mundipharma. Sebastian Böttcher: research funding from Janssen and AbbVie; and honoraria from Roche, Janssen, AbbVie, Novartis, Becton Dickinson, AstraZeneca, and Sanofi. Wolfram Klapper: Research grants from Roche, Amgen, Janssen, InCyte Regeneraon, Takeda and advisory role (Roche) paid to my institution. All without relevance for the current manuscript. Barbara Eichhorst: Consultant or advisory board member, research support or travel support by AbbVie, AstraZeneca, Celgene, F. Hoffmann-LaRoche, Gilead, Janssen-Cilag.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


