{"title":"Venetoclax 联合多柔比星和阿糖胞苷(2 + 6)治疗急性髓性白血病:II期试验的最新结果。","authors":"Xiaohui Suo, Zheng Fang, Dongmei Wang, Liyun Zhao, Jie Liu, Hong Li, Xiaojun Ma, Congcong Zhang, Xuemei Zhao, Rui Shi, Yan Wu, Zongjiu Jiao, Jiaojie Song, Ling Zhang, Ling Li, Suping Zhang, Xinxiao Lu, Linyu Yuan, Sifeng Gao, Jilei Zhang, Kaiqi Liu, Xingli Zhao, Guanchen Bai, Yingchang Mi","doi":"10.1002/hon.3296","DOIUrl":null,"url":null,"abstract":"<p>Previous research has demonstrated that the combination of Venetoclax (Ven) and intensive chemotherapy (IC) enhances the complete response (CR) and minimal residual disease (MRD) negative rate in patients with de novo Acute Myeloid Leukemia (AML).<span><sup>1-5</sup></span> Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy for AML patients.<span><sup>1</sup></span> The objective of this data update is to further substantiate the efficacy and safety of this induction regimen.</p><p>Until 30 Nov 2023, 85 patients were enrolled in this study. Baseline characteristics of 85 patients are in Table S1. According to the ELN 2022 risk classification, 37 (43.5%), 13 (15.3%), and 35 (41.2%) patients belonged to the favorable, intermediate, and adverse groups, respectively.</p><p>After one cycle induction therapy, the overall response rate (ORR, CR + CRi + PR) was 94.1% (80/85) with a composite complete response rate (cCR, CR + CRi) of 91.8% (78/85) and 85.7% (60/70) of the patients reached cCR with MRD (−) by flow cytometry. The cCR rate was 97.3% (36/37) in patients with ELN (2022) favorable risk, 84.6% (11/13) in patients with intermediate risk, and 88.6% (31/35) in patients with adverse risk (Table 1). The adverse effects and recovery time of blood cells consistent with our previous reports. Tumor lysis syndrome was only observed in one patient, and one patient died during induction therapy.</p><p>Until 30 Jan 2024, with a median follow-up of 12 (0.5–24) months, eleven (11/84, 13.1%) patients underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT). The estimated 12-month overall survival (OS), event-free survival (EFS) and disease-free survival (DFS) rates were 82.2%, 81.9%, 82.7%, respectively (Figure S1). According to the 2022 ELN prognostic risk classification, the estimated 12-month OS, EFS, and DFS rates were 93.5% (95% CI: 88.3%–98.6%), 93.3% (95% CI: 88.1%–98.5%), and 93.3% (95% CI: 84.3%–100%), respectively, in favorable risk group; 91.7% (95% CI: 86.6%–96.8%), 90.0% (95% CI: 84.7%–95.3%), 90.9% (95% CI: 73.8%–100%), respectively, for intermediate-risk patients; and 64.6% (95% CI: 44.4%–84.8%), 62.9% (95% CI: 41.9%–83.9%), and 64.9% (95% CI: 43.7%–86.1%), respectively for adverse-risk patients (Figure 1).</p><p>Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy. To further corroborate our previous results, we extended the study to continue enrolled patients and continue follow-up of earlier patients.</p><p>The updated results are shown that the ORR after one cycle of induction was 94.1% (80/85) with a cCR rate of 91.8% (78/85) and MRD (−) rate 85.7%. The rates of cCR, MRD negativity, and recovery time for neutrophils and PLT counts were consistent with our previous report. The results further substantiate the efficacy and safety of our induction regimen. In comparison to previous reports,<span><sup>2, 4, 5</sup></span> our induction therapy yielded a significantly reduced duration of myelo-suppression while maintaining comparable efficacy.</p><p>In this report, the estimated 12-month OS, EFS, and DFS rates were 82.2%, 81.9%, and 82.7% respectively, with a median follow-up of 12 (0.5–24) months. Specifically, the 12-month OS, EFS and DFS of patients who classified as low and intermediate risk groups exceeded 90%. These results are encouraging considering that the proportion (13.1%, 11/84) of patients who underwent allo-HSCT in our study was significantly lower than previously reported.<span><sup>2, 4, 5</sup></span> This will facilitate the further optimization of treatment protocols for newly diagnosed AML patients. This outcome may be attributed to several factors: (1) this regimen is the first to integrate Ven with induction, consolidation, and maintenance therapy. Combination of Ven and IC as an induction therapy significantly improved the cCR and MRD (−) rates, thereby establishing a robust foundation for long-term survival. (2) Both induction and consolidation therapy were well-tolerated and good compliance in comparison to Kadia TM and DiNardo CD's reports,<span><sup>4, 5</sup></span> and treatment was consistently administered according to the prescribed regimen in majority of patients. (3) The maintenance therapy based on Ven combined with AZA may potentially reduce disease relapse and improve the OS.</p><p>The results of the data update show that Ven combined with DA (2 + 6) is a safe and highly effective induction therapy for patients with newly diagnosed AML. Long-term survival benefits require longer follow-up.</p><p><b>Yingchang Mi</b> and <b>Kaiqi Liu</b> designed the study. <b>Xiaohui Suo</b>, <b>Fang Zheng</b>, <b>Xingli Zhao</b> and <b>Guanchen Bai</b> were participated in therapeutic regimen discussion. <b>Xiaohui Suo</b> and <b>Kaiqi Liu</b> collected the data, and wrote the first draft. <b>Hong Li</b> analyzed the data. <b>Xiaohui Suo</b>, <b>Fang Zheng</b>, <b>Dongmei Wang</b>, <b>Liyun Zhao</b>, <b>Jie Liu</b>, <b>Hong Li</b>, <b>Xiaojun Ma</b>, <b>Congcong Zhang</b>, <b>Xuemei Zhao</b>, <b>Rui Shi</b>, <b>Yan Wu</b>, <b>Zongjiu Jiao</b>, <b>Jiaojie Song</b>, <b>Ling Zhang</b>, <b>Ling Li</b>, <b>Suping Zhang</b>, <b>Xinxiao Lu</b>, <b>Linyu Yuan</b>, <b>Sifeng Gao</b>, <b>Jilei Zhang</b>, <b>Kaiqi Liu</b>, <b>Xingli Zhao</b>, <b>Guanchen Bai</b>, <b>Yingchang Mi</b> were involved in patient management, follow up and clinical data collection. <b>Yingchang Mi</b> and <b>Kaiqi Liu</b> revised the manuscript. All authors read and approved the final manuscript. ALL authors had full access to all the data and had final responsibility for the decision to submit for publication.</p><p>This work was supported by grant 82270190 from the National Natural Science Foundation of China (NSFC); Tianjin Key Medical Discipline (Specialty) Construction Project (Grant No.TJYXZDXK-053B); Special project for research and development ability of colleges and universities (22422083037ZC, Handan Science and Technology Bureau); Shandong Society of Geriatrics 2021 Annual science and technology Development Plan project No (LKJGG2021W120).</p><p>The authors have no conflicts of interest to declare.</p><p>All studies involving human participants were meticulously reviewed and approved by the relevant institutional and national research committee(s), adhering to the ethical standards set forth in the Helsinki Declaration (as revised in 2013). Informed consent was obtained from the patients' parents or guardians.</p><p>All authors have reviewed and given their approval for the manuscript's publication.</p>","PeriodicalId":12882,"journal":{"name":"Hematological Oncology","volume":"42 4","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2024-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3296","citationCount":"0","resultStr":"{\"title\":\"Venetoclax combined with daunorubicin and cytarabine (2 + 6) in acute myeloid leukemia: Updated results of a phase II trial\",\"authors\":\"Xiaohui Suo, Zheng Fang, Dongmei Wang, Liyun Zhao, Jie Liu, Hong Li, Xiaojun Ma, Congcong Zhang, Xuemei Zhao, Rui Shi, Yan Wu, Zongjiu Jiao, Jiaojie Song, Ling Zhang, Ling Li, Suping Zhang, Xinxiao Lu, Linyu Yuan, Sifeng Gao, Jilei Zhang, Kaiqi Liu, Xingli Zhao, Guanchen Bai, Yingchang Mi\",\"doi\":\"10.1002/hon.3296\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Previous research has demonstrated that the combination of Venetoclax (Ven) and intensive chemotherapy (IC) enhances the complete response (CR) and minimal residual disease (MRD) negative rate in patients with de novo Acute Myeloid Leukemia (AML).<span><sup>1-5</sup></span> Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy for AML patients.<span><sup>1</sup></span> The objective of this data update is to further substantiate the efficacy and safety of this induction regimen.</p><p>Until 30 Nov 2023, 85 patients were enrolled in this study. Baseline characteristics of 85 patients are in Table S1. According to the ELN 2022 risk classification, 37 (43.5%), 13 (15.3%), and 35 (41.2%) patients belonged to the favorable, intermediate, and adverse groups, respectively.</p><p>After one cycle induction therapy, the overall response rate (ORR, CR + CRi + PR) was 94.1% (80/85) with a composite complete response rate (cCR, CR + CRi) of 91.8% (78/85) and 85.7% (60/70) of the patients reached cCR with MRD (−) by flow cytometry. The cCR rate was 97.3% (36/37) in patients with ELN (2022) favorable risk, 84.6% (11/13) in patients with intermediate risk, and 88.6% (31/35) in patients with adverse risk (Table 1). The adverse effects and recovery time of blood cells consistent with our previous reports. Tumor lysis syndrome was only observed in one patient, and one patient died during induction therapy.</p><p>Until 30 Jan 2024, with a median follow-up of 12 (0.5–24) months, eleven (11/84, 13.1%) patients underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT). The estimated 12-month overall survival (OS), event-free survival (EFS) and disease-free survival (DFS) rates were 82.2%, 81.9%, 82.7%, respectively (Figure S1). According to the 2022 ELN prognostic risk classification, the estimated 12-month OS, EFS, and DFS rates were 93.5% (95% CI: 88.3%–98.6%), 93.3% (95% CI: 88.1%–98.5%), and 93.3% (95% CI: 84.3%–100%), respectively, in favorable risk group; 91.7% (95% CI: 86.6%–96.8%), 90.0% (95% CI: 84.7%–95.3%), 90.9% (95% CI: 73.8%–100%), respectively, for intermediate-risk patients; and 64.6% (95% CI: 44.4%–84.8%), 62.9% (95% CI: 41.9%–83.9%), and 64.9% (95% CI: 43.7%–86.1%), respectively for adverse-risk patients (Figure 1).</p><p>Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy. To further corroborate our previous results, we extended the study to continue enrolled patients and continue follow-up of earlier patients.</p><p>The updated results are shown that the ORR after one cycle of induction was 94.1% (80/85) with a cCR rate of 91.8% (78/85) and MRD (−) rate 85.7%. The rates of cCR, MRD negativity, and recovery time for neutrophils and PLT counts were consistent with our previous report. The results further substantiate the efficacy and safety of our induction regimen. In comparison to previous reports,<span><sup>2, 4, 5</sup></span> our induction therapy yielded a significantly reduced duration of myelo-suppression while maintaining comparable efficacy.</p><p>In this report, the estimated 12-month OS, EFS, and DFS rates were 82.2%, 81.9%, and 82.7% respectively, with a median follow-up of 12 (0.5–24) months. Specifically, the 12-month OS, EFS and DFS of patients who classified as low and intermediate risk groups exceeded 90%. These results are encouraging considering that the proportion (13.1%, 11/84) of patients who underwent allo-HSCT in our study was significantly lower than previously reported.<span><sup>2, 4, 5</sup></span> This will facilitate the further optimization of treatment protocols for newly diagnosed AML patients. This outcome may be attributed to several factors: (1) this regimen is the first to integrate Ven with induction, consolidation, and maintenance therapy. Combination of Ven and IC as an induction therapy significantly improved the cCR and MRD (−) rates, thereby establishing a robust foundation for long-term survival. (2) Both induction and consolidation therapy were well-tolerated and good compliance in comparison to Kadia TM and DiNardo CD's reports,<span><sup>4, 5</sup></span> and treatment was consistently administered according to the prescribed regimen in majority of patients. (3) The maintenance therapy based on Ven combined with AZA may potentially reduce disease relapse and improve the OS.</p><p>The results of the data update show that Ven combined with DA (2 + 6) is a safe and highly effective induction therapy for patients with newly diagnosed AML. Long-term survival benefits require longer follow-up.</p><p><b>Yingchang Mi</b> and <b>Kaiqi Liu</b> designed the study. <b>Xiaohui Suo</b>, <b>Fang Zheng</b>, <b>Xingli Zhao</b> and <b>Guanchen Bai</b> were participated in therapeutic regimen discussion. <b>Xiaohui Suo</b> and <b>Kaiqi Liu</b> collected the data, and wrote the first draft. <b>Hong Li</b> analyzed the data. <b>Xiaohui Suo</b>, <b>Fang Zheng</b>, <b>Dongmei Wang</b>, <b>Liyun Zhao</b>, <b>Jie Liu</b>, <b>Hong Li</b>, <b>Xiaojun Ma</b>, <b>Congcong Zhang</b>, <b>Xuemei Zhao</b>, <b>Rui Shi</b>, <b>Yan Wu</b>, <b>Zongjiu Jiao</b>, <b>Jiaojie Song</b>, <b>Ling Zhang</b>, <b>Ling Li</b>, <b>Suping Zhang</b>, <b>Xinxiao Lu</b>, <b>Linyu Yuan</b>, <b>Sifeng Gao</b>, <b>Jilei Zhang</b>, <b>Kaiqi Liu</b>, <b>Xingli Zhao</b>, <b>Guanchen Bai</b>, <b>Yingchang Mi</b> were involved in patient management, follow up and clinical data collection. <b>Yingchang Mi</b> and <b>Kaiqi Liu</b> revised the manuscript. All authors read and approved the final manuscript. ALL authors had full access to all the data and had final responsibility for the decision to submit for publication.</p><p>This work was supported by grant 82270190 from the National Natural Science Foundation of China (NSFC); Tianjin Key Medical Discipline (Specialty) Construction Project (Grant No.TJYXZDXK-053B); Special project for research and development ability of colleges and universities (22422083037ZC, Handan Science and Technology Bureau); Shandong Society of Geriatrics 2021 Annual science and technology Development Plan project No (LKJGG2021W120).</p><p>The authors have no conflicts of interest to declare.</p><p>All studies involving human participants were meticulously reviewed and approved by the relevant institutional and national research committee(s), adhering to the ethical standards set forth in the Helsinki Declaration (as revised in 2013). Informed consent was obtained from the patients' parents or guardians.</p><p>All authors have reviewed and given their approval for the manuscript's publication.</p>\",\"PeriodicalId\":12882,\"journal\":{\"name\":\"Hematological Oncology\",\"volume\":\"42 4\",\"pages\":\"\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3296\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematological Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hon.3296\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematological Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hon.3296","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Venetoclax combined with daunorubicin and cytarabine (2 + 6) in acute myeloid leukemia: Updated results of a phase II trial
Previous research has demonstrated that the combination of Venetoclax (Ven) and intensive chemotherapy (IC) enhances the complete response (CR) and minimal residual disease (MRD) negative rate in patients with de novo Acute Myeloid Leukemia (AML).1-5 Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy for AML patients.1 The objective of this data update is to further substantiate the efficacy and safety of this induction regimen.
Until 30 Nov 2023, 85 patients were enrolled in this study. Baseline characteristics of 85 patients are in Table S1. According to the ELN 2022 risk classification, 37 (43.5%), 13 (15.3%), and 35 (41.2%) patients belonged to the favorable, intermediate, and adverse groups, respectively.
After one cycle induction therapy, the overall response rate (ORR, CR + CRi + PR) was 94.1% (80/85) with a composite complete response rate (cCR, CR + CRi) of 91.8% (78/85) and 85.7% (60/70) of the patients reached cCR with MRD (−) by flow cytometry. The cCR rate was 97.3% (36/37) in patients with ELN (2022) favorable risk, 84.6% (11/13) in patients with intermediate risk, and 88.6% (31/35) in patients with adverse risk (Table 1). The adverse effects and recovery time of blood cells consistent with our previous reports. Tumor lysis syndrome was only observed in one patient, and one patient died during induction therapy.
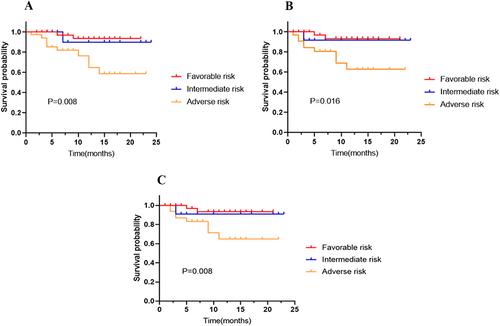
Until 30 Jan 2024, with a median follow-up of 12 (0.5–24) months, eleven (11/84, 13.1%) patients underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT). The estimated 12-month overall survival (OS), event-free survival (EFS) and disease-free survival (DFS) rates were 82.2%, 81.9%, 82.7%, respectively (Figure S1). According to the 2022 ELN prognostic risk classification, the estimated 12-month OS, EFS, and DFS rates were 93.5% (95% CI: 88.3%–98.6%), 93.3% (95% CI: 88.1%–98.5%), and 93.3% (95% CI: 84.3%–100%), respectively, in favorable risk group; 91.7% (95% CI: 86.6%–96.8%), 90.0% (95% CI: 84.7%–95.3%), 90.9% (95% CI: 73.8%–100%), respectively, for intermediate-risk patients; and 64.6% (95% CI: 44.4%–84.8%), 62.9% (95% CI: 41.9%–83.9%), and 64.9% (95% CI: 43.7%–86.1%), respectively for adverse-risk patients (Figure 1).
Our previous study showed that Ven combined with DA (2 + 6) is a highly effective and safe induction therapy. To further corroborate our previous results, we extended the study to continue enrolled patients and continue follow-up of earlier patients.
The updated results are shown that the ORR after one cycle of induction was 94.1% (80/85) with a cCR rate of 91.8% (78/85) and MRD (−) rate 85.7%. The rates of cCR, MRD negativity, and recovery time for neutrophils and PLT counts were consistent with our previous report. The results further substantiate the efficacy and safety of our induction regimen. In comparison to previous reports,2, 4, 5 our induction therapy yielded a significantly reduced duration of myelo-suppression while maintaining comparable efficacy.
In this report, the estimated 12-month OS, EFS, and DFS rates were 82.2%, 81.9%, and 82.7% respectively, with a median follow-up of 12 (0.5–24) months. Specifically, the 12-month OS, EFS and DFS of patients who classified as low and intermediate risk groups exceeded 90%. These results are encouraging considering that the proportion (13.1%, 11/84) of patients who underwent allo-HSCT in our study was significantly lower than previously reported.2, 4, 5 This will facilitate the further optimization of treatment protocols for newly diagnosed AML patients. This outcome may be attributed to several factors: (1) this regimen is the first to integrate Ven with induction, consolidation, and maintenance therapy. Combination of Ven and IC as an induction therapy significantly improved the cCR and MRD (−) rates, thereby establishing a robust foundation for long-term survival. (2) Both induction and consolidation therapy were well-tolerated and good compliance in comparison to Kadia TM and DiNardo CD's reports,4, 5 and treatment was consistently administered according to the prescribed regimen in majority of patients. (3) The maintenance therapy based on Ven combined with AZA may potentially reduce disease relapse and improve the OS.
The results of the data update show that Ven combined with DA (2 + 6) is a safe and highly effective induction therapy for patients with newly diagnosed AML. Long-term survival benefits require longer follow-up.
Yingchang Mi and Kaiqi Liu designed the study. Xiaohui Suo, Fang Zheng, Xingli Zhao and Guanchen Bai were participated in therapeutic regimen discussion. Xiaohui Suo and Kaiqi Liu collected the data, and wrote the first draft. Hong Li analyzed the data. Xiaohui Suo, Fang Zheng, Dongmei Wang, Liyun Zhao, Jie Liu, Hong Li, Xiaojun Ma, Congcong Zhang, Xuemei Zhao, Rui Shi, Yan Wu, Zongjiu Jiao, Jiaojie Song, Ling Zhang, Ling Li, Suping Zhang, Xinxiao Lu, Linyu Yuan, Sifeng Gao, Jilei Zhang, Kaiqi Liu, Xingli Zhao, Guanchen Bai, Yingchang Mi were involved in patient management, follow up and clinical data collection. Yingchang Mi and Kaiqi Liu revised the manuscript. All authors read and approved the final manuscript. ALL authors had full access to all the data and had final responsibility for the decision to submit for publication.
This work was supported by grant 82270190 from the National Natural Science Foundation of China (NSFC); Tianjin Key Medical Discipline (Specialty) Construction Project (Grant No.TJYXZDXK-053B); Special project for research and development ability of colleges and universities (22422083037ZC, Handan Science and Technology Bureau); Shandong Society of Geriatrics 2021 Annual science and technology Development Plan project No (LKJGG2021W120).
The authors have no conflicts of interest to declare.
All studies involving human participants were meticulously reviewed and approved by the relevant institutional and national research committee(s), adhering to the ethical standards set forth in the Helsinki Declaration (as revised in 2013). Informed consent was obtained from the patients' parents or guardians.
All authors have reviewed and given their approval for the manuscript's publication.
期刊介绍:
Hematological Oncology considers for publication articles dealing with experimental and clinical aspects of neoplastic diseases of the hemopoietic and lymphoid systems and relevant related matters. Translational studies applying basic science to clinical issues are particularly welcomed. Manuscripts dealing with the following areas are encouraged:
-Clinical practice and management of hematological neoplasia, including: acute and chronic leukemias, malignant lymphomas, myeloproliferative disorders
-Diagnostic investigations, including imaging and laboratory assays
-Epidemiology, pathology and pathobiology of hematological neoplasia of hematological diseases
-Therapeutic issues including Phase 1, 2 or 3 trials as well as allogeneic and autologous stem cell transplantation studies
-Aspects of the cell biology, molecular biology, molecular genetics and cytogenetics of normal or diseased hematopoeisis and lymphopoiesis, including stem cells and cytokines and other regulatory systems.
Concise, topical review material is welcomed, especially if it makes new concepts and ideas accessible to a wider community. Proposals for review material may be discussed with the Editor-in-Chief. Collections of case material and case reports will be considered only if they have broader scientific or clinical relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


