Anne Klausing, Kristina Waschk, Frederick Far, Markus Martini, Franz-Josef Kramer
{"title":"肿瘤风险评分(TRS)--头颈部肿瘤手术的下一级风险预测。","authors":"Anne Klausing, Kristina Waschk, Frederick Far, Markus Martini, Franz-Josef Kramer","doi":"10.1007/s10006-024-01281-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Head and neck cancer surgery often requires postoperative monitoring in an intensive care unit (ICU) or intermediate care unit (IMC). With a variety of different risk scores, it is incumbent upon the investigator to plan a risk-adapted allocation of resources. Tumor surgery in the head and neck region itself offers a wide range of procedures in terms of resection extent and reconstruction methods, which can be stratified only vaguely by a cross-disciplinary score. Facing a variety of different risk scores we aimed to develop a new Tumor Risk Score (TRS) enabling anterograde preoperative risk evaluation, resource allocation and optimization of cost and outcome measurements in tumor surgery of the head and neck.</p><p><strong>Methods: </strong>A collective of 547 patients (2010-2021) with intraoral tumors was studied to develop the TRS by grading the preoperative tumor size and location as well as the invasiveness of the planned surgery by means of statistical modeling. Two postoperative complications were defined: (1) prolonged postoperative stay in IMC/ICU and (2) prolonged total length of stay (LOS). Each parameter was analyzed using TRS and all preoperative patient parameters (age, sex, preoperative hemoglobin, body-mass-index, preexisting medical conditions) using predictive modeling design. Established risk scores (Charlson Comorbidity Index (CCI), American Society of Anesthesiologists risk classification (ASA), Functional Comorbidity Index (FCI)) and Patient Clinical Complexity Level (PCCL) were used as benchmarks for model performance of the TRS.</p><p><strong>Results: </strong>The TRS is significantly correlated with surgery duration (p < 0.001) and LOS (p = 0.001). With every increase in TRS, LOS rises by 9.3% (95%CI 4.7-13.9; p < 0.001) or 1.9 days (95%CI 1.0-2.8; p < 0.001), respectively. For each increase in TRS, the LOS in IMC/ICU wards increases by 0.33 days (95%CI 0.12-0.54; p = 0.002), and the probability of an overall prolonged IMC/ICU stay increased by 32.3% per TRS class (p < 0.001). Exceeding the planned IMC/ICU LOS, overall LOS increased by 7.7 days (95%CI 5.35-10.08; p < 0.001) and increases the likelihood of also exceeding the upper limit LOS by 70.1% (95%CI 1.02-2.85; p = 0.041). In terms of predictive power of a prolonged IMC/ICU stay, the TRS performs better than previously established risk scores such as ASA or CCI (p = 0.031).</p><p><strong>Conclusion: </strong>The lack of a standardized needs assessment can lead to both under- and overutilization of the IMC/ICU and therefore increased costs and losses in total revenue. Our index helps to stratify the risk of a prolonged IMC/ICU stay preoperatively and to adjust resource allocation in major head and neck tumor surgery.</p>","PeriodicalId":47251,"journal":{"name":"Oral and Maxillofacial Surgery-Heidelberg","volume":" ","pages":"1547-1556"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11480139/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Tumor Risk Score (TRS) - next level risk prediction in head and neck tumor surgery.\",\"authors\":\"Anne Klausing, Kristina Waschk, Frederick Far, Markus Martini, Franz-Josef Kramer\",\"doi\":\"10.1007/s10006-024-01281-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Head and neck cancer surgery often requires postoperative monitoring in an intensive care unit (ICU) or intermediate care unit (IMC). With a variety of different risk scores, it is incumbent upon the investigator to plan a risk-adapted allocation of resources. Tumor surgery in the head and neck region itself offers a wide range of procedures in terms of resection extent and reconstruction methods, which can be stratified only vaguely by a cross-disciplinary score. Facing a variety of different risk scores we aimed to develop a new Tumor Risk Score (TRS) enabling anterograde preoperative risk evaluation, resource allocation and optimization of cost and outcome measurements in tumor surgery of the head and neck.</p><p><strong>Methods: </strong>A collective of 547 patients (2010-2021) with intraoral tumors was studied to develop the TRS by grading the preoperative tumor size and location as well as the invasiveness of the planned surgery by means of statistical modeling. Two postoperative complications were defined: (1) prolonged postoperative stay in IMC/ICU and (2) prolonged total length of stay (LOS). Each parameter was analyzed using TRS and all preoperative patient parameters (age, sex, preoperative hemoglobin, body-mass-index, preexisting medical conditions) using predictive modeling design. Established risk scores (Charlson Comorbidity Index (CCI), American Society of Anesthesiologists risk classification (ASA), Functional Comorbidity Index (FCI)) and Patient Clinical Complexity Level (PCCL) were used as benchmarks for model performance of the TRS.</p><p><strong>Results: </strong>The TRS is significantly correlated with surgery duration (p < 0.001) and LOS (p = 0.001). With every increase in TRS, LOS rises by 9.3% (95%CI 4.7-13.9; p < 0.001) or 1.9 days (95%CI 1.0-2.8; p < 0.001), respectively. For each increase in TRS, the LOS in IMC/ICU wards increases by 0.33 days (95%CI 0.12-0.54; p = 0.002), and the probability of an overall prolonged IMC/ICU stay increased by 32.3% per TRS class (p < 0.001). Exceeding the planned IMC/ICU LOS, overall LOS increased by 7.7 days (95%CI 5.35-10.08; p < 0.001) and increases the likelihood of also exceeding the upper limit LOS by 70.1% (95%CI 1.02-2.85; p = 0.041). In terms of predictive power of a prolonged IMC/ICU stay, the TRS performs better than previously established risk scores such as ASA or CCI (p = 0.031).</p><p><strong>Conclusion: </strong>The lack of a standardized needs assessment can lead to both under- and overutilization of the IMC/ICU and therefore increased costs and losses in total revenue. Our index helps to stratify the risk of a prolonged IMC/ICU stay preoperatively and to adjust resource allocation in major head and neck tumor surgery.</p>\",\"PeriodicalId\":47251,\"journal\":{\"name\":\"Oral and Maxillofacial Surgery-Heidelberg\",\"volume\":\" \",\"pages\":\"1547-1556\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11480139/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Oral and Maxillofacial Surgery-Heidelberg\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s10006-024-01281-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oral and Maxillofacial Surgery-Heidelberg","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10006-024-01281-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
The Tumor Risk Score (TRS) - next level risk prediction in head and neck tumor surgery.
Purpose: Head and neck cancer surgery often requires postoperative monitoring in an intensive care unit (ICU) or intermediate care unit (IMC). With a variety of different risk scores, it is incumbent upon the investigator to plan a risk-adapted allocation of resources. Tumor surgery in the head and neck region itself offers a wide range of procedures in terms of resection extent and reconstruction methods, which can be stratified only vaguely by a cross-disciplinary score. Facing a variety of different risk scores we aimed to develop a new Tumor Risk Score (TRS) enabling anterograde preoperative risk evaluation, resource allocation and optimization of cost and outcome measurements in tumor surgery of the head and neck.
Methods: A collective of 547 patients (2010-2021) with intraoral tumors was studied to develop the TRS by grading the preoperative tumor size and location as well as the invasiveness of the planned surgery by means of statistical modeling. Two postoperative complications were defined: (1) prolonged postoperative stay in IMC/ICU and (2) prolonged total length of stay (LOS). Each parameter was analyzed using TRS and all preoperative patient parameters (age, sex, preoperative hemoglobin, body-mass-index, preexisting medical conditions) using predictive modeling design. Established risk scores (Charlson Comorbidity Index (CCI), American Society of Anesthesiologists risk classification (ASA), Functional Comorbidity Index (FCI)) and Patient Clinical Complexity Level (PCCL) were used as benchmarks for model performance of the TRS.
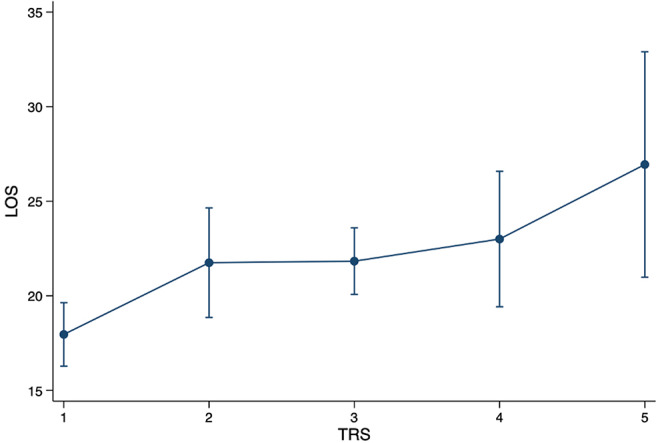
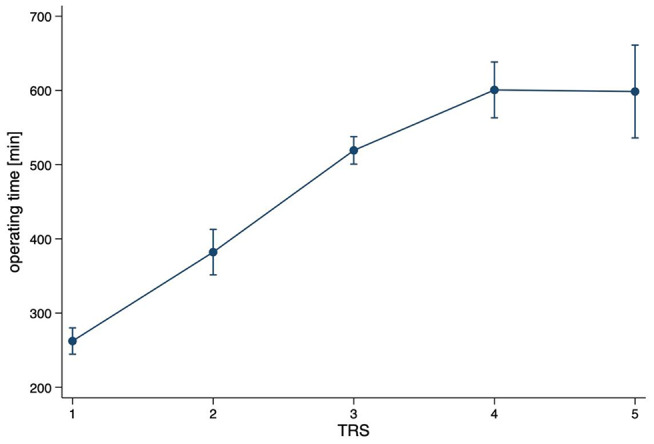
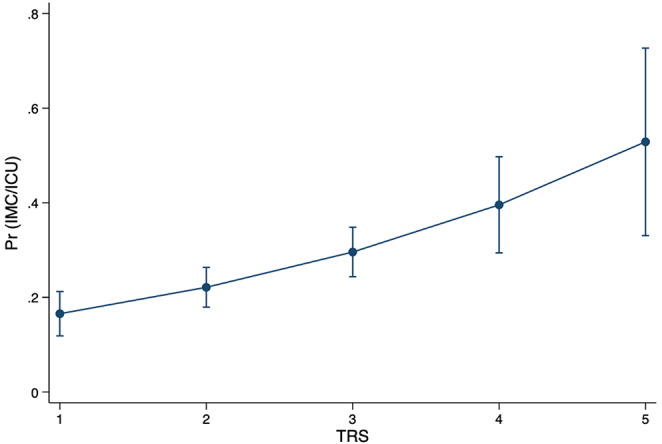
Results: The TRS is significantly correlated with surgery duration (p < 0.001) and LOS (p = 0.001). With every increase in TRS, LOS rises by 9.3% (95%CI 4.7-13.9; p < 0.001) or 1.9 days (95%CI 1.0-2.8; p < 0.001), respectively. For each increase in TRS, the LOS in IMC/ICU wards increases by 0.33 days (95%CI 0.12-0.54; p = 0.002), and the probability of an overall prolonged IMC/ICU stay increased by 32.3% per TRS class (p < 0.001). Exceeding the planned IMC/ICU LOS, overall LOS increased by 7.7 days (95%CI 5.35-10.08; p < 0.001) and increases the likelihood of also exceeding the upper limit LOS by 70.1% (95%CI 1.02-2.85; p = 0.041). In terms of predictive power of a prolonged IMC/ICU stay, the TRS performs better than previously established risk scores such as ASA or CCI (p = 0.031).
Conclusion: The lack of a standardized needs assessment can lead to both under- and overutilization of the IMC/ICU and therefore increased costs and losses in total revenue. Our index helps to stratify the risk of a prolonged IMC/ICU stay preoperatively and to adjust resource allocation in major head and neck tumor surgery.
期刊介绍:
Oral & Maxillofacial Surgery founded as Mund-, Kiefer- und Gesichtschirurgie is a peer-reviewed online journal. It is designed for clinicians as well as researchers.The quarterly journal offers comprehensive coverage of new techniques, important developments and innovative ideas in oral and maxillofacial surgery and interdisciplinary aspects of cranial, facial and oral diseases and their management. The journal publishes papers of the highest scientific merit and widest possible scope on work in oral and maxillofacial surgery as well as supporting specialties. Practice-oriented articles help improve the methods used in oral and maxillofacial surgery.Every aspect of oral and maxillofacial surgery is fully covered through a range of invited review articles, clinical and research articles, technical notes, abstracts, and case reports. Specific topics are: aesthetic facial surgery, clinical pathology, computer-assisted surgery, congenital and craniofacial deformities, dentoalveolar surgery, head and neck oncology, implant dentistry, oral medicine, orthognathic surgery, reconstructive surgery, skull base surgery, TMJ and trauma.Time-limited reviewing and electronic processing allow to publish articles as fast as possible. Accepted articles are rapidly accessible online.Clinical studies submitted for publication have to include a declaration that they have been approved by an ethical committee according to the World Medical Association Declaration of Helsinki 1964 (last amendment during the 52nd World Medical Association General Assembly, Edinburgh, Scotland, October 2000). Experimental animal studies have to be carried out according to the principles of laboratory animal care (NIH publication No 86-23, revised 1985).
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


