Charlotte Mund, Katharina Asmus, Wajima Safi, Oliver Ritter, Dominique Petrus, Susann Patschan, Daniel Patschan
{"title":"临床上明显的心肺功能不明显影响化脓性急性肾损伤患者的预后。","authors":"Charlotte Mund, Katharina Asmus, Wajima Safi, Oliver Ritter, Dominique Petrus, Susann Patschan, Daniel Patschan","doi":"10.14740/jocmr5190","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is a common issue among in-hospital patients, with high mortality rates. Sepsis is a primary cause of AKI, particularly in the intensive care unit. Patients with septic AKI often experience cardiovascular congestion, leading to the formal classification of cardiorenal syndrome type 5. The study aimed to evaluate the prognosis of septic AKI patients with and without clinical evidence of cardiovascular congestion.</p><p><strong>Methods: </strong>This was a retrospective observational study. AKI patients were identified using the in-hospital AKI alert system. Sepsis was diagnosed based on laboratory, clinical, and hemodynamic characteristics, with additional consideration of the quickSOFA score. Cardiovascular congestion was diagnosed by assessing clinical (edema), radiographic (pulmonary congestion), echocardiographic (e.g., wall motion abnormalities), and laboratory variables (e.g., N-terminal pro-B-type natriuretic peptide). Endpoints included in-hospital survival, the need for kidney replacement therapy (KRT), and recovery of kidney function (ROKF).</p><p><strong>Results: </strong>In total, 102 patients were included, and cardiopulmonary congestion was diagnosed in 78.4%. Individuals with congestion did not differ from patients without congestion in any of the pre-defined endpoints.</p><p><strong>Conclusions: </strong>It is justified not to consider clinically apparent cardiovascular congestion in septic AKI patients as a risk factor for death <i>per se</i>. Rather, especially in the case of sepsis, clinically apparent positive fluid balance does not seem to be a disadvantage in terms of survival, KRT, and ROKF.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 6","pages":"302-309"},"PeriodicalIF":2.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11254307/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinically Evident Cardiopulmonary Congestion Does Not Significantly Impact the Prognosis of Patients With Septic Acute Kidney Injury.\",\"authors\":\"Charlotte Mund, Katharina Asmus, Wajima Safi, Oliver Ritter, Dominique Petrus, Susann Patschan, Daniel Patschan\",\"doi\":\"10.14740/jocmr5190\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute kidney injury (AKI) is a common issue among in-hospital patients, with high mortality rates. Sepsis is a primary cause of AKI, particularly in the intensive care unit. Patients with septic AKI often experience cardiovascular congestion, leading to the formal classification of cardiorenal syndrome type 5. The study aimed to evaluate the prognosis of septic AKI patients with and without clinical evidence of cardiovascular congestion.</p><p><strong>Methods: </strong>This was a retrospective observational study. AKI patients were identified using the in-hospital AKI alert system. Sepsis was diagnosed based on laboratory, clinical, and hemodynamic characteristics, with additional consideration of the quickSOFA score. Cardiovascular congestion was diagnosed by assessing clinical (edema), radiographic (pulmonary congestion), echocardiographic (e.g., wall motion abnormalities), and laboratory variables (e.g., N-terminal pro-B-type natriuretic peptide). Endpoints included in-hospital survival, the need for kidney replacement therapy (KRT), and recovery of kidney function (ROKF).</p><p><strong>Results: </strong>In total, 102 patients were included, and cardiopulmonary congestion was diagnosed in 78.4%. Individuals with congestion did not differ from patients without congestion in any of the pre-defined endpoints.</p><p><strong>Conclusions: </strong>It is justified not to consider clinically apparent cardiovascular congestion in septic AKI patients as a risk factor for death <i>per se</i>. Rather, especially in the case of sepsis, clinically apparent positive fluid balance does not seem to be a disadvantage in terms of survival, KRT, and ROKF.</p>\",\"PeriodicalId\":94329,\"journal\":{\"name\":\"Journal of clinical medicine research\",\"volume\":\"16 6\",\"pages\":\"302-309\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11254307/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of clinical medicine research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr5190\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr5190","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:急性肾损伤(AKI)是院内患者的常见病,死亡率很高。脓毒症是导致急性肾损伤的主要原因,尤其是在重症监护病房。脓毒症急性肾损伤患者通常会出现心血管充血,因此被正式划分为心肾综合征 5 型。本研究旨在评估有和无心血管充血临床证据的脓毒性 AKI 患者的预后:这是一项回顾性观察研究。通过院内 AKI 警报系统识别 AKI 患者。根据实验室、临床和血流动力学特征诊断败血症,并额外考虑 quickSOFA 评分。通过评估临床(水肿)、影像学(肺充血)、超声心动图(如室壁运动异常)和实验室变量(如N末端前B型钠尿肽)来诊断心血管充血。终点包括院内存活率、肾脏替代疗法(KRT)需求和肾功能恢复(ROKF):共纳入 102 名患者,78.4% 的患者被诊断为心肺充血。结果:共纳入 102 名患者,78.4% 的患者被诊断为心肺充血,在任何预设终点上,充血患者与无充血患者均无差异:结论:脓毒症 AKI 患者临床上明显的心血管充血本身并不是死亡的危险因素。相反,尤其是在脓毒症患者中,临床上明显的正液体平衡似乎并不会对患者的存活率、KRT 和 ROKF 造成不利影响。
Clinically Evident Cardiopulmonary Congestion Does Not Significantly Impact the Prognosis of Patients With Septic Acute Kidney Injury.
Background: Acute kidney injury (AKI) is a common issue among in-hospital patients, with high mortality rates. Sepsis is a primary cause of AKI, particularly in the intensive care unit. Patients with septic AKI often experience cardiovascular congestion, leading to the formal classification of cardiorenal syndrome type 5. The study aimed to evaluate the prognosis of septic AKI patients with and without clinical evidence of cardiovascular congestion.
Methods: This was a retrospective observational study. AKI patients were identified using the in-hospital AKI alert system. Sepsis was diagnosed based on laboratory, clinical, and hemodynamic characteristics, with additional consideration of the quickSOFA score. Cardiovascular congestion was diagnosed by assessing clinical (edema), radiographic (pulmonary congestion), echocardiographic (e.g., wall motion abnormalities), and laboratory variables (e.g., N-terminal pro-B-type natriuretic peptide). Endpoints included in-hospital survival, the need for kidney replacement therapy (KRT), and recovery of kidney function (ROKF).
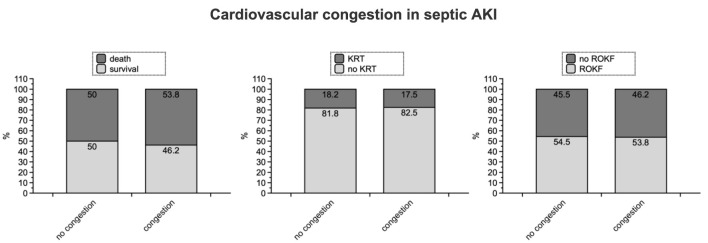
Results: In total, 102 patients were included, and cardiopulmonary congestion was diagnosed in 78.4%. Individuals with congestion did not differ from patients without congestion in any of the pre-defined endpoints.
Conclusions: It is justified not to consider clinically apparent cardiovascular congestion in septic AKI patients as a risk factor for death per se. Rather, especially in the case of sepsis, clinically apparent positive fluid balance does not seem to be a disadvantage in terms of survival, KRT, and ROKF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


