Ke Li Chow , Paula Elizabeth Keating , Kamal Solanki , Mark Sapsford , Karen Lindsay , John Liston O'Donnell
{"title":"抗-HMGCR肌病:新西兰全国队列中临床表现的多样性","authors":"Ke Li Chow , Paula Elizabeth Keating , Kamal Solanki , Mark Sapsford , Karen Lindsay , John Liston O'Donnell","doi":"10.1016/j.semarthrit.2024.152522","DOIUrl":null,"url":null,"abstract":"<div><h3>Aims</h3><p>We describe the varied clinical presentations, barriers in diagnosis and outcomes of anti-HMGCR myopathy in a large national cohort.</p></div><div><h3>Methods</h3><p>Adults found positive for serum anti-HMGCR autoantibodies via line blot or enzyme-immunoassay followed by immunoprecipitation were included in the study.</p></div><div><h3>Results</h3><p>Of 75 patients identified, the records of 72 (96 %) described weakness as the presenting symptom. The records of 65 gave a reliable description of proximal weakness. In 22/65 (33.8 %) the weakness was described as predominantly or solely lower limb weakness. Forty-five of 75 (60 %) presented with a subacute onset (duration of symptoms >4 weeks -≤6 months), whilst 22/75 (29.3 %) presented with a more indolent chronic onset (duration of symptoms >6 months). Eighteen of 75 (24 %) suffered falls and 2/75 (2.7 %) had “general decline”. In three patients no weakness was described: two presented with myalgia and one with a skin rash characterized as Jessner lymphocytic skin rash. Median creatine kinase at presentation was 7337 U/L (range 1050–25,500). Muscle biopsy was performed in 38 (50.7 %). Associated malignancy was infrequent. Four patients recovered without immunosuppression. Five-year and 10-year survival was 92.7 % (95 % CI 80.6–97.4 %), and 82.5 % (95 % CI 61.2–92.8 %) respectively.</p></div><div><h3>Conclusion</h3><p>Recurrent falls, a long prodrome and dominant lower limb proximal weakness were common in this anti-HMGCR myopathy cohort. These features overlap with frailty syndrome and sporadic inclusion body myositis emphasizing the importance of considering anti-HMGCR myopathy in that clinical context. A minority of patients recover after statin withdrawal alone.</p></div>","PeriodicalId":21715,"journal":{"name":"Seminars in arthritis and rheumatism","volume":"68 ","pages":"Article 152522"},"PeriodicalIF":4.6000,"publicationDate":"2024-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Anti-HMGCR myopathy: Diversity of clinical presentations in a national cohort in New Zealand\",\"authors\":\"Ke Li Chow , Paula Elizabeth Keating , Kamal Solanki , Mark Sapsford , Karen Lindsay , John Liston O'Donnell\",\"doi\":\"10.1016/j.semarthrit.2024.152522\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Aims</h3><p>We describe the varied clinical presentations, barriers in diagnosis and outcomes of anti-HMGCR myopathy in a large national cohort.</p></div><div><h3>Methods</h3><p>Adults found positive for serum anti-HMGCR autoantibodies via line blot or enzyme-immunoassay followed by immunoprecipitation were included in the study.</p></div><div><h3>Results</h3><p>Of 75 patients identified, the records of 72 (96 %) described weakness as the presenting symptom. The records of 65 gave a reliable description of proximal weakness. In 22/65 (33.8 %) the weakness was described as predominantly or solely lower limb weakness. Forty-five of 75 (60 %) presented with a subacute onset (duration of symptoms >4 weeks -≤6 months), whilst 22/75 (29.3 %) presented with a more indolent chronic onset (duration of symptoms >6 months). Eighteen of 75 (24 %) suffered falls and 2/75 (2.7 %) had “general decline”. In three patients no weakness was described: two presented with myalgia and one with a skin rash characterized as Jessner lymphocytic skin rash. Median creatine kinase at presentation was 7337 U/L (range 1050–25,500). Muscle biopsy was performed in 38 (50.7 %). Associated malignancy was infrequent. Four patients recovered without immunosuppression. Five-year and 10-year survival was 92.7 % (95 % CI 80.6–97.4 %), and 82.5 % (95 % CI 61.2–92.8 %) respectively.</p></div><div><h3>Conclusion</h3><p>Recurrent falls, a long prodrome and dominant lower limb proximal weakness were common in this anti-HMGCR myopathy cohort. These features overlap with frailty syndrome and sporadic inclusion body myositis emphasizing the importance of considering anti-HMGCR myopathy in that clinical context. A minority of patients recover after statin withdrawal alone.</p></div>\",\"PeriodicalId\":21715,\"journal\":{\"name\":\"Seminars in arthritis and rheumatism\",\"volume\":\"68 \",\"pages\":\"Article 152522\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-07-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in arthritis and rheumatism\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0049017224001628\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in arthritis and rheumatism","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0049017224001628","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
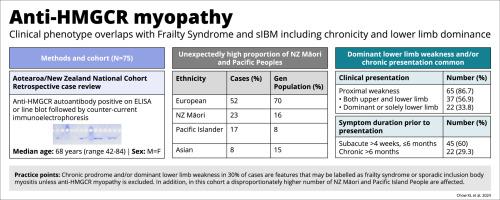
Anti-HMGCR myopathy: Diversity of clinical presentations in a national cohort in New Zealand
Aims
We describe the varied clinical presentations, barriers in diagnosis and outcomes of anti-HMGCR myopathy in a large national cohort.
Methods
Adults found positive for serum anti-HMGCR autoantibodies via line blot or enzyme-immunoassay followed by immunoprecipitation were included in the study.
Results
Of 75 patients identified, the records of 72 (96 %) described weakness as the presenting symptom. The records of 65 gave a reliable description of proximal weakness. In 22/65 (33.8 %) the weakness was described as predominantly or solely lower limb weakness. Forty-five of 75 (60 %) presented with a subacute onset (duration of symptoms >4 weeks -≤6 months), whilst 22/75 (29.3 %) presented with a more indolent chronic onset (duration of symptoms >6 months). Eighteen of 75 (24 %) suffered falls and 2/75 (2.7 %) had “general decline”. In three patients no weakness was described: two presented with myalgia and one with a skin rash characterized as Jessner lymphocytic skin rash. Median creatine kinase at presentation was 7337 U/L (range 1050–25,500). Muscle biopsy was performed in 38 (50.7 %). Associated malignancy was infrequent. Four patients recovered without immunosuppression. Five-year and 10-year survival was 92.7 % (95 % CI 80.6–97.4 %), and 82.5 % (95 % CI 61.2–92.8 %) respectively.
Conclusion
Recurrent falls, a long prodrome and dominant lower limb proximal weakness were common in this anti-HMGCR myopathy cohort. These features overlap with frailty syndrome and sporadic inclusion body myositis emphasizing the importance of considering anti-HMGCR myopathy in that clinical context. A minority of patients recover after statin withdrawal alone.
期刊介绍:
Seminars in Arthritis and Rheumatism provides access to the highest-quality clinical, therapeutic and translational research about arthritis, rheumatology and musculoskeletal disorders that affect the joints and connective tissue. Each bimonthly issue includes articles giving you the latest diagnostic criteria, consensus statements, systematic reviews and meta-analyses as well as clinical and translational research studies. Read this journal for the latest groundbreaking research and to gain insights from scientists and clinicians on the management and treatment of musculoskeletal and autoimmune rheumatologic diseases. The journal is of interest to rheumatologists, orthopedic surgeons, internal medicine physicians, immunologists and specialists in bone and mineral metabolism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


