Christopher Shwei Wen Tham, Jeffrey Quek, Yeh Ching Linn, Lawrence Ng, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan, Thuan Tong Tan, Hein Than
{"title":"2019年造血干细胞移植期间急性冠状病毒疾病的影响--来自真实世界临床实践的经验","authors":"Christopher Shwei Wen Tham, Jeffrey Quek, Yeh Ching Linn, Lawrence Ng, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan, Thuan Tong Tan, Hein Than","doi":"10.1002/jha2.978","DOIUrl":null,"url":null,"abstract":"<p>The impact of community-acquired respiratory viral infections (CARVIs) in the transplant population has been highlighted by the recent coronavirus disease 2019 (COVID-19) pandemic. Patients undergoing haematopoietic stem cell transplantation (HCT) following acute COVID-19 experienced significant morbidity and mortality. Few guidelines and reports suggest that HCT is deferred during persistent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positivity during and after infection, and is feasible only in fully recovered patients [<span>1, 2</span>]. However, those with high-risk haematological malignancies often progress and succumb to their disease without timely HCT. These two opposing pressures must therefore be reconciled, yet data are sparse on the optimal timing and safety of HCT that needs be performed during or immediately following acute COVID-19 infection.</p><p>In this study at Singapore General Hospital, the largest tertiary transplant centre in Singapore, the outcome of patients who underwent HCT following COVID-19 in the preceding 120 days or with active COVID-19 infection during transplant was analysed. A retrospective analysis of transplant-related outcomes in consecutive patients admitted for planned HCT between September 2021 and April 2022 was conducted. COVID-19 was detected by SARS-CoV-2 RNA by polymerase chain reaction (PCR) on nasopharyngeal swab. Patients diagnosed with COVID-19 within 120 days prior to stem cell infusion were included in the study.</p><p>We identified 10 allogeneic and 1 autologous HCT patients. Median interval between diagnosis of COVID-19 to HCT infusion was 53 days (range 1–118). Median duration of COVID-19 infection (defined by time to negative PCR) was 20 days. Six patients tested negative by PCR and 2 were prolonged low-level viral shedders, prior to HCT. Two patients were diagnosed with COVID-19 while receiving conditioning chemotherapy prior to HCT infusion, at days −1 and −3, respectively.</p><p>All allogeneic HCT patients were fully vaccinated with two doses of mRNA vaccines (Pfizer-BioNTech BNT162b2 or Moderna mRNA-1273) prior to infection. Median receptor binding domain IgG serology titre (Abbott assay) in vaccinated patients was 1301 AU/mL at the time of COVID-19 diagnosis. COVID-19 disease severity by National Institutes of Health (NIH) guidelines [<span>3</span>] was mild in nine patients, moderate in one patient and critical in one patient. Eight patients received antivirals with or without concurrent monoclonal antibodies (mab; sotrovimab, <i>n</i> = 4; casirivimab–imdevimab, <i>n</i> = 1).</p><p>Patient characteristics and outcomes are summarised in Table 1, and transplant-related details are provided in Supporting Information Table 1. Two patients died of non-relapse pulmonary complications on days +43 and +50 post-HCT. There were no instances of grade III–IV acute graft versus host disease and no evidence of SARS-CoV-2 reinfection or late complications, or increase in viral reactivation of cytomegalovirus, Epstein-Barr virus and human herpesvirus 6.</p><p>Two patients with COVID-19 infection immediately prior to HCT were promptly treated with antiviral and/or mab, but experienced diverse clinical courses as illustrated in Figure 1. Patient 5 who had haplo-identical HCT with post-transplant cyclophosphamide (PTCy) was diagnosed with COVID-19 infection 3 days prior to stem cell infusion. He developed severe COVID-19 pneumonia on day +7 post-transplant and eventually died on day +50 from respiratory failure. In contrast, patient 4 who had relatively low exposure to immunosuppressive chemotherapy had uncomplicated COVID-19 clinical course without lower respiratory tract infection, despite acquiring infection 1 day prior to stem cell infusion and lasting 20 days.</p><p>Existing evidence addresses the outcomes of patients who develop COVID-19 after HCT, rather than immediately preceding or during transplant. Prospective data suggest that COVID-19 is more likely to lead to lower respiratory tract infection and mortality in those post-HCT [<span>4, 5</span>]. It is also noteworthy that these studies looked at earlier variants of SARS-CoV-2 when vaccination and therapeutics were not widely established. There is minimal data and guidance on the optimal timing of HCT post-COVID-19 or the treatment of COVID-19 during HCT.</p><p>Optimising patients prior to HCT is crucial in the context of unpredictable risk of CARVIs. Vaccination, if available, should remain the mainstay of pre-emptive therapy. Although there is no international consensus on how to determine immunogenicity post-vaccination for COVID-19 during the pandemic, neutralising antibody titre was one correlate of protection [<span>9</span>], which was used at our centre. Those with lymphoid malignancies or receiving lymphodepleting treatment, particularly anti-CD20 therapy, may have a reduced titre of the neutralising antibody, suboptimal efficacy of vaccination, and prolonged viral shedding [<span>6</span>]. Among the patients who died in our cohort, we observed a trend for lower absolute lymphocyte counts (ALC) (median 0.7, range 0.42–0.98 × 10<sup>9</sup>/L) at the start of transplant preparative regimen, compared to the ALC in those who remained alive (median 1.5, range: 0–7.16 × 10<sup>9</sup>/L).</p><p>T cells also play an essential role in protective immunity against COVID-19 [<span>7</span>], typically later on in the disease process once cells have been infected and start to present viral antigens, as compared to the antibody response. However, this aspect of immune function is not readily assessable in routine clinical practice. This is particularly important for those undergoing haploidentical HCT, either with in vivo PTCy administration or ex vivo T-cell depletion of the graft. The intended immunosuppressive effect of PTCy on alloreactive host T cells is likely to affect the immune system's ability to combat COVID-19, resulting in delayed viral clearance and severe pneumonia, as seen in patient 5 of our cohort.</p><p>Persistence of SARS-CoV-2 RNA in lung tissue has been demonstrated, even after being undetectable on nasopharyngeal swab. In one published case, digital PCR analysis of lung samples post mortem was positive for SARS-CoV-2 [<span>8</span>], and in another, was detected on bronchoalveolar lavage specimens as well as immunohistochemistry of lung samples [<span>9</span>]. Patient 3 in our cohort, who had an undetectable SARS-CoV-2 RNA by PCR at the time of transplant, died 43 days post-HCT from complications related to idiopathic pneumonia syndrome. We hypothesise that lung injury from COVID-19 may have predisposed to this rare post-transplant complication, though there is limited data in the literature regarding this at present.</p><p>Overall, our study suggests that timely and life-saving HCT requires cautious monitoring and comprehensive supportive care including vaccination and early anti-viral therapy of for acute COVID-19 infection peri-transplant. It is important to highlight the potential mortality that can arise from pulmonary complications post-COVID-19, as with two cases in our cohort. Furthermore, a careful decision on conditioning regimens with T-cell depletion should be made according to disease risk–benefit assessment. The potential effect of COVID-19 on long-term post-transplant outcomes, such as GvHD and immune-mediated complications, warrants continued evaluation.</p><p>Christopher Shwei Wen Tham designed the research study, performed data collection, analysis and wrote the paper. Hein Than designed the research study, analysed the data and wrote the paper.</p><p>Yeh Ching Linn, Lawrence Ng, Jeffrey Quek, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan and Thuan Tong Tan contributed to research study design, provided the data, and were responsible for critical review and editing of the manuscript.</p><p>The authors declare no conflicts of interest.</p><p>The authors received no specific funding for this work.</p><p>The authors have confirmed ethical approval statement is not needed for this submission.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>Not applicable.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 4","pages":"907-910"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.978","citationCount":"0","resultStr":"{\"title\":\"Implications of acute coronavirus disease 2019 during haematopoietic stem cell transplantation—Experience from real-world clinical practice\",\"authors\":\"Christopher Shwei Wen Tham, Jeffrey Quek, Yeh Ching Linn, Lawrence Ng, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan, Thuan Tong Tan, Hein Than\",\"doi\":\"10.1002/jha2.978\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The impact of community-acquired respiratory viral infections (CARVIs) in the transplant population has been highlighted by the recent coronavirus disease 2019 (COVID-19) pandemic. Patients undergoing haematopoietic stem cell transplantation (HCT) following acute COVID-19 experienced significant morbidity and mortality. Few guidelines and reports suggest that HCT is deferred during persistent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positivity during and after infection, and is feasible only in fully recovered patients [<span>1, 2</span>]. However, those with high-risk haematological malignancies often progress and succumb to their disease without timely HCT. These two opposing pressures must therefore be reconciled, yet data are sparse on the optimal timing and safety of HCT that needs be performed during or immediately following acute COVID-19 infection.</p><p>In this study at Singapore General Hospital, the largest tertiary transplant centre in Singapore, the outcome of patients who underwent HCT following COVID-19 in the preceding 120 days or with active COVID-19 infection during transplant was analysed. A retrospective analysis of transplant-related outcomes in consecutive patients admitted for planned HCT between September 2021 and April 2022 was conducted. COVID-19 was detected by SARS-CoV-2 RNA by polymerase chain reaction (PCR) on nasopharyngeal swab. Patients diagnosed with COVID-19 within 120 days prior to stem cell infusion were included in the study.</p><p>We identified 10 allogeneic and 1 autologous HCT patients. Median interval between diagnosis of COVID-19 to HCT infusion was 53 days (range 1–118). Median duration of COVID-19 infection (defined by time to negative PCR) was 20 days. Six patients tested negative by PCR and 2 were prolonged low-level viral shedders, prior to HCT. Two patients were diagnosed with COVID-19 while receiving conditioning chemotherapy prior to HCT infusion, at days −1 and −3, respectively.</p><p>All allogeneic HCT patients were fully vaccinated with two doses of mRNA vaccines (Pfizer-BioNTech BNT162b2 or Moderna mRNA-1273) prior to infection. Median receptor binding domain IgG serology titre (Abbott assay) in vaccinated patients was 1301 AU/mL at the time of COVID-19 diagnosis. COVID-19 disease severity by National Institutes of Health (NIH) guidelines [<span>3</span>] was mild in nine patients, moderate in one patient and critical in one patient. Eight patients received antivirals with or without concurrent monoclonal antibodies (mab; sotrovimab, <i>n</i> = 4; casirivimab–imdevimab, <i>n</i> = 1).</p><p>Patient characteristics and outcomes are summarised in Table 1, and transplant-related details are provided in Supporting Information Table 1. Two patients died of non-relapse pulmonary complications on days +43 and +50 post-HCT. There were no instances of grade III–IV acute graft versus host disease and no evidence of SARS-CoV-2 reinfection or late complications, or increase in viral reactivation of cytomegalovirus, Epstein-Barr virus and human herpesvirus 6.</p><p>Two patients with COVID-19 infection immediately prior to HCT were promptly treated with antiviral and/or mab, but experienced diverse clinical courses as illustrated in Figure 1. Patient 5 who had haplo-identical HCT with post-transplant cyclophosphamide (PTCy) was diagnosed with COVID-19 infection 3 days prior to stem cell infusion. He developed severe COVID-19 pneumonia on day +7 post-transplant and eventually died on day +50 from respiratory failure. In contrast, patient 4 who had relatively low exposure to immunosuppressive chemotherapy had uncomplicated COVID-19 clinical course without lower respiratory tract infection, despite acquiring infection 1 day prior to stem cell infusion and lasting 20 days.</p><p>Existing evidence addresses the outcomes of patients who develop COVID-19 after HCT, rather than immediately preceding or during transplant. Prospective data suggest that COVID-19 is more likely to lead to lower respiratory tract infection and mortality in those post-HCT [<span>4, 5</span>]. It is also noteworthy that these studies looked at earlier variants of SARS-CoV-2 when vaccination and therapeutics were not widely established. There is minimal data and guidance on the optimal timing of HCT post-COVID-19 or the treatment of COVID-19 during HCT.</p><p>Optimising patients prior to HCT is crucial in the context of unpredictable risk of CARVIs. Vaccination, if available, should remain the mainstay of pre-emptive therapy. Although there is no international consensus on how to determine immunogenicity post-vaccination for COVID-19 during the pandemic, neutralising antibody titre was one correlate of protection [<span>9</span>], which was used at our centre. Those with lymphoid malignancies or receiving lymphodepleting treatment, particularly anti-CD20 therapy, may have a reduced titre of the neutralising antibody, suboptimal efficacy of vaccination, and prolonged viral shedding [<span>6</span>]. Among the patients who died in our cohort, we observed a trend for lower absolute lymphocyte counts (ALC) (median 0.7, range 0.42–0.98 × 10<sup>9</sup>/L) at the start of transplant preparative regimen, compared to the ALC in those who remained alive (median 1.5, range: 0–7.16 × 10<sup>9</sup>/L).</p><p>T cells also play an essential role in protective immunity against COVID-19 [<span>7</span>], typically later on in the disease process once cells have been infected and start to present viral antigens, as compared to the antibody response. However, this aspect of immune function is not readily assessable in routine clinical practice. This is particularly important for those undergoing haploidentical HCT, either with in vivo PTCy administration or ex vivo T-cell depletion of the graft. The intended immunosuppressive effect of PTCy on alloreactive host T cells is likely to affect the immune system's ability to combat COVID-19, resulting in delayed viral clearance and severe pneumonia, as seen in patient 5 of our cohort.</p><p>Persistence of SARS-CoV-2 RNA in lung tissue has been demonstrated, even after being undetectable on nasopharyngeal swab. In one published case, digital PCR analysis of lung samples post mortem was positive for SARS-CoV-2 [<span>8</span>], and in another, was detected on bronchoalveolar lavage specimens as well as immunohistochemistry of lung samples [<span>9</span>]. Patient 3 in our cohort, who had an undetectable SARS-CoV-2 RNA by PCR at the time of transplant, died 43 days post-HCT from complications related to idiopathic pneumonia syndrome. We hypothesise that lung injury from COVID-19 may have predisposed to this rare post-transplant complication, though there is limited data in the literature regarding this at present.</p><p>Overall, our study suggests that timely and life-saving HCT requires cautious monitoring and comprehensive supportive care including vaccination and early anti-viral therapy of for acute COVID-19 infection peri-transplant. It is important to highlight the potential mortality that can arise from pulmonary complications post-COVID-19, as with two cases in our cohort. Furthermore, a careful decision on conditioning regimens with T-cell depletion should be made according to disease risk–benefit assessment. The potential effect of COVID-19 on long-term post-transplant outcomes, such as GvHD and immune-mediated complications, warrants continued evaluation.</p><p>Christopher Shwei Wen Tham designed the research study, performed data collection, analysis and wrote the paper. Hein Than designed the research study, analysed the data and wrote the paper.</p><p>Yeh Ching Linn, Lawrence Ng, Jeffrey Quek, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan and Thuan Tong Tan contributed to research study design, provided the data, and were responsible for critical review and editing of the manuscript.</p><p>The authors declare no conflicts of interest.</p><p>The authors received no specific funding for this work.</p><p>The authors have confirmed ethical approval statement is not needed for this submission.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>Not applicable.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>\",\"PeriodicalId\":72883,\"journal\":{\"name\":\"EJHaem\",\"volume\":\"5 4\",\"pages\":\"907-910\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-07-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.978\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EJHaem\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jha2.978\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.978","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Implications of acute coronavirus disease 2019 during haematopoietic stem cell transplantation—Experience from real-world clinical practice
The impact of community-acquired respiratory viral infections (CARVIs) in the transplant population has been highlighted by the recent coronavirus disease 2019 (COVID-19) pandemic. Patients undergoing haematopoietic stem cell transplantation (HCT) following acute COVID-19 experienced significant morbidity and mortality. Few guidelines and reports suggest that HCT is deferred during persistent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positivity during and after infection, and is feasible only in fully recovered patients [1, 2]. However, those with high-risk haematological malignancies often progress and succumb to their disease without timely HCT. These two opposing pressures must therefore be reconciled, yet data are sparse on the optimal timing and safety of HCT that needs be performed during or immediately following acute COVID-19 infection.
In this study at Singapore General Hospital, the largest tertiary transplant centre in Singapore, the outcome of patients who underwent HCT following COVID-19 in the preceding 120 days or with active COVID-19 infection during transplant was analysed. A retrospective analysis of transplant-related outcomes in consecutive patients admitted for planned HCT between September 2021 and April 2022 was conducted. COVID-19 was detected by SARS-CoV-2 RNA by polymerase chain reaction (PCR) on nasopharyngeal swab. Patients diagnosed with COVID-19 within 120 days prior to stem cell infusion were included in the study.
We identified 10 allogeneic and 1 autologous HCT patients. Median interval between diagnosis of COVID-19 to HCT infusion was 53 days (range 1–118). Median duration of COVID-19 infection (defined by time to negative PCR) was 20 days. Six patients tested negative by PCR and 2 were prolonged low-level viral shedders, prior to HCT. Two patients were diagnosed with COVID-19 while receiving conditioning chemotherapy prior to HCT infusion, at days −1 and −3, respectively.
All allogeneic HCT patients were fully vaccinated with two doses of mRNA vaccines (Pfizer-BioNTech BNT162b2 or Moderna mRNA-1273) prior to infection. Median receptor binding domain IgG serology titre (Abbott assay) in vaccinated patients was 1301 AU/mL at the time of COVID-19 diagnosis. COVID-19 disease severity by National Institutes of Health (NIH) guidelines [3] was mild in nine patients, moderate in one patient and critical in one patient. Eight patients received antivirals with or without concurrent monoclonal antibodies (mab; sotrovimab, n = 4; casirivimab–imdevimab, n = 1).
Patient characteristics and outcomes are summarised in Table 1, and transplant-related details are provided in Supporting Information Table 1. Two patients died of non-relapse pulmonary complications on days +43 and +50 post-HCT. There were no instances of grade III–IV acute graft versus host disease and no evidence of SARS-CoV-2 reinfection or late complications, or increase in viral reactivation of cytomegalovirus, Epstein-Barr virus and human herpesvirus 6.
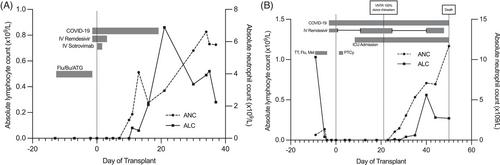
Two patients with COVID-19 infection immediately prior to HCT were promptly treated with antiviral and/or mab, but experienced diverse clinical courses as illustrated in Figure 1. Patient 5 who had haplo-identical HCT with post-transplant cyclophosphamide (PTCy) was diagnosed with COVID-19 infection 3 days prior to stem cell infusion. He developed severe COVID-19 pneumonia on day +7 post-transplant and eventually died on day +50 from respiratory failure. In contrast, patient 4 who had relatively low exposure to immunosuppressive chemotherapy had uncomplicated COVID-19 clinical course without lower respiratory tract infection, despite acquiring infection 1 day prior to stem cell infusion and lasting 20 days.
Existing evidence addresses the outcomes of patients who develop COVID-19 after HCT, rather than immediately preceding or during transplant. Prospective data suggest that COVID-19 is more likely to lead to lower respiratory tract infection and mortality in those post-HCT [4, 5]. It is also noteworthy that these studies looked at earlier variants of SARS-CoV-2 when vaccination and therapeutics were not widely established. There is minimal data and guidance on the optimal timing of HCT post-COVID-19 or the treatment of COVID-19 during HCT.
Optimising patients prior to HCT is crucial in the context of unpredictable risk of CARVIs. Vaccination, if available, should remain the mainstay of pre-emptive therapy. Although there is no international consensus on how to determine immunogenicity post-vaccination for COVID-19 during the pandemic, neutralising antibody titre was one correlate of protection [9], which was used at our centre. Those with lymphoid malignancies or receiving lymphodepleting treatment, particularly anti-CD20 therapy, may have a reduced titre of the neutralising antibody, suboptimal efficacy of vaccination, and prolonged viral shedding [6]. Among the patients who died in our cohort, we observed a trend for lower absolute lymphocyte counts (ALC) (median 0.7, range 0.42–0.98 × 109/L) at the start of transplant preparative regimen, compared to the ALC in those who remained alive (median 1.5, range: 0–7.16 × 109/L).
T cells also play an essential role in protective immunity against COVID-19 [7], typically later on in the disease process once cells have been infected and start to present viral antigens, as compared to the antibody response. However, this aspect of immune function is not readily assessable in routine clinical practice. This is particularly important for those undergoing haploidentical HCT, either with in vivo PTCy administration or ex vivo T-cell depletion of the graft. The intended immunosuppressive effect of PTCy on alloreactive host T cells is likely to affect the immune system's ability to combat COVID-19, resulting in delayed viral clearance and severe pneumonia, as seen in patient 5 of our cohort.
Persistence of SARS-CoV-2 RNA in lung tissue has been demonstrated, even after being undetectable on nasopharyngeal swab. In one published case, digital PCR analysis of lung samples post mortem was positive for SARS-CoV-2 [8], and in another, was detected on bronchoalveolar lavage specimens as well as immunohistochemistry of lung samples [9]. Patient 3 in our cohort, who had an undetectable SARS-CoV-2 RNA by PCR at the time of transplant, died 43 days post-HCT from complications related to idiopathic pneumonia syndrome. We hypothesise that lung injury from COVID-19 may have predisposed to this rare post-transplant complication, though there is limited data in the literature regarding this at present.
Overall, our study suggests that timely and life-saving HCT requires cautious monitoring and comprehensive supportive care including vaccination and early anti-viral therapy of for acute COVID-19 infection peri-transplant. It is important to highlight the potential mortality that can arise from pulmonary complications post-COVID-19, as with two cases in our cohort. Furthermore, a careful decision on conditioning regimens with T-cell depletion should be made according to disease risk–benefit assessment. The potential effect of COVID-19 on long-term post-transplant outcomes, such as GvHD and immune-mediated complications, warrants continued evaluation.
Christopher Shwei Wen Tham designed the research study, performed data collection, analysis and wrote the paper. Hein Than designed the research study, analysed the data and wrote the paper.
Yeh Ching Linn, Lawrence Ng, Jeffrey Quek, Aloysius Ho, Francesca Lim, Yunxin Chen, Chandramouli Nagarajan, William Hwang, Jing Jing Lee, Gina Gan, Shimin Jasmine Chung, Ban Hock Tan and Thuan Tong Tan contributed to research study design, provided the data, and were responsible for critical review and editing of the manuscript.
The authors declare no conflicts of interest.
The authors received no specific funding for this work.
The authors have confirmed ethical approval statement is not needed for this submission.
The authors have confirmed patient consent statement is not needed for this submission.
Not applicable.
The authors have confirmed clinical trial registration is not needed for this submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


