Morgan Pooler MD, Andrew T. Reiter MD, Joseph S. Colla MD
{"title":"患有高血压和腹痛的男子","authors":"Morgan Pooler MD, Andrew T. Reiter MD, Joseph S. Colla MD","doi":"10.1002/emp2.13230","DOIUrl":null,"url":null,"abstract":"<p>A 61-year-old with history of hypertension and atrial flutter on rivaroxaban presented to the emergency department from a cardiology clinic for uncontrolled hypertension. The patient reported intermittent, nonexertional, left-sided chest, and epigastric pressure. On examination, the patient had elevated blood pressure: left arm 240/131 and right arm 217/109. Vital signs were otherwise normal and physical examination was unremarkable. The patient's electrocardiogram showed no acute ischemic changes. Point-of-care ultrasound (Video 1 and Figure 1) and computed tomography angiography (CTA) (Figure 2) of the patient's aorta were obtained.</p><p>Spontaneous isolated celiac artery dissection (SICAD) is a rare visceral arterial dissection, the second leading type after superior mesenteric artery dissection. Symptoms can range from an asymptomatic incidental finding to severe epigastric, back, or flank pain in middle-aged adults.<span><sup>1, 2</sup></span> The most prevalent risk factors include male sex, smoking, and hypertension.<span><sup>3, 4</sup></span> CTA is the primary modality used to diagnose SICAD worldwide. Findings include an intimal flap, which is pathognomonic, or a mural thrombus in the celiac lumen. Complications include organ ischemia, aneurysm formation, and rupture.<span><sup>5</sup></span> First-line treatment for SICAD is conservative management including strict blood pressure control, antithrombotic therapy, and surveillance. Surgical and endovascular intervention are reserved for patients who have failed conservative treatment.<span><sup>6</sup></span></p><p>Our patient was admitted to the cardiac intensive care unit on a labetalol drip to treat hypertensive emergency. Vascular surgery was consulted and recommended addition of a daily aspirin and atorvastatin to his home medications and smoking cessation. The patient was discharged home in stable condition on hospital day 2.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":null,"pages":null},"PeriodicalIF":1.6000,"publicationDate":"2024-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13230","citationCount":"0","resultStr":"{\"title\":\"Man with hypertension and abdominal pain\",\"authors\":\"Morgan Pooler MD, Andrew T. Reiter MD, Joseph S. Colla MD\",\"doi\":\"10.1002/emp2.13230\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 61-year-old with history of hypertension and atrial flutter on rivaroxaban presented to the emergency department from a cardiology clinic for uncontrolled hypertension. The patient reported intermittent, nonexertional, left-sided chest, and epigastric pressure. On examination, the patient had elevated blood pressure: left arm 240/131 and right arm 217/109. Vital signs were otherwise normal and physical examination was unremarkable. The patient's electrocardiogram showed no acute ischemic changes. Point-of-care ultrasound (Video 1 and Figure 1) and computed tomography angiography (CTA) (Figure 2) of the patient's aorta were obtained.</p><p>Spontaneous isolated celiac artery dissection (SICAD) is a rare visceral arterial dissection, the second leading type after superior mesenteric artery dissection. Symptoms can range from an asymptomatic incidental finding to severe epigastric, back, or flank pain in middle-aged adults.<span><sup>1, 2</sup></span> The most prevalent risk factors include male sex, smoking, and hypertension.<span><sup>3, 4</sup></span> CTA is the primary modality used to diagnose SICAD worldwide. Findings include an intimal flap, which is pathognomonic, or a mural thrombus in the celiac lumen. Complications include organ ischemia, aneurysm formation, and rupture.<span><sup>5</sup></span> First-line treatment for SICAD is conservative management including strict blood pressure control, antithrombotic therapy, and surveillance. Surgical and endovascular intervention are reserved for patients who have failed conservative treatment.<span><sup>6</sup></span></p><p>Our patient was admitted to the cardiac intensive care unit on a labetalol drip to treat hypertensive emergency. Vascular surgery was consulted and recommended addition of a daily aspirin and atorvastatin to his home medications and smoking cessation. The patient was discharged home in stable condition on hospital day 2.</p>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13230\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13230\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13230","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
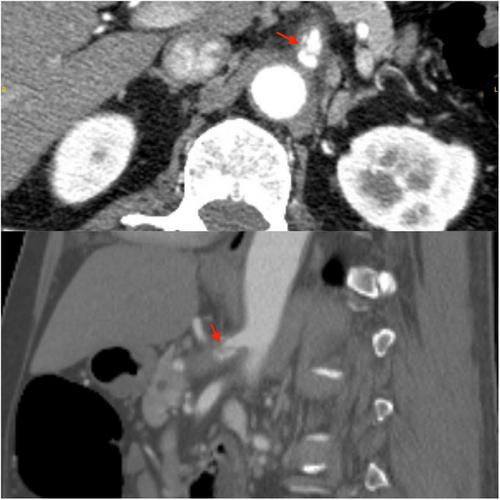
A 61-year-old with history of hypertension and atrial flutter on rivaroxaban presented to the emergency department from a cardiology clinic for uncontrolled hypertension. The patient reported intermittent, nonexertional, left-sided chest, and epigastric pressure. On examination, the patient had elevated blood pressure: left arm 240/131 and right arm 217/109. Vital signs were otherwise normal and physical examination was unremarkable. The patient's electrocardiogram showed no acute ischemic changes. Point-of-care ultrasound (Video 1 and Figure 1) and computed tomography angiography (CTA) (Figure 2) of the patient's aorta were obtained.
Spontaneous isolated celiac artery dissection (SICAD) is a rare visceral arterial dissection, the second leading type after superior mesenteric artery dissection. Symptoms can range from an asymptomatic incidental finding to severe epigastric, back, or flank pain in middle-aged adults.1, 2 The most prevalent risk factors include male sex, smoking, and hypertension.3, 4 CTA is the primary modality used to diagnose SICAD worldwide. Findings include an intimal flap, which is pathognomonic, or a mural thrombus in the celiac lumen. Complications include organ ischemia, aneurysm formation, and rupture.5 First-line treatment for SICAD is conservative management including strict blood pressure control, antithrombotic therapy, and surveillance. Surgical and endovascular intervention are reserved for patients who have failed conservative treatment.6
Our patient was admitted to the cardiac intensive care unit on a labetalol drip to treat hypertensive emergency. Vascular surgery was consulted and recommended addition of a daily aspirin and atorvastatin to his home medications and smoking cessation. The patient was discharged home in stable condition on hospital day 2.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


