Simeon Schietzel, Sarah Jane Rippin Wagner, Luzia Nigg Calanca
{"title":"腹膜透析中的腹膜炎:何时考虑急性胰腺炎?病例报告和微型综述。","authors":"Simeon Schietzel, Sarah Jane Rippin Wagner, Luzia Nigg Calanca","doi":"10.1159/000539185","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute pancreatitis is an infrequent but challenging cause of peritonitis in peritoneal dialysis (PD). Presentation is often indistinguishable from infectious peritonitis, interpretation of pancreatic enzymes is not straight-forward, and multiple etiologies need to be considered.</p><p><strong>Case presentation: </strong>A 74-year-old PD patient presented with cloudy dialysate and subtle symptoms of malaise and abdominal pain. WBC was 26,000/µL, CRP was 250 mg/L, and dialysis effluent contained 1,047 leucocytes/μL (90% polymorphs). Infectious peritonitis was presumed, and antibiotic treatment started. However, dialysate cultures remained negative, effluent leucocyte count remained high, and clinical condition deteriorated. Abdominal ultrasound was unremarkable (pancreas not visible). Acute pancreatitis was diagnosed by elevated lipase level (serum: 628 U/L, dialysis fluid: 15 U/L) and CT scan. Disentangling etiological factors was challenging. The patient had gallstones, consumed alcoholic beverages, was recently on doxycycline and dialyzed with icodextrin. In addition, PD treatment itself may have been a contributory factor. Antibiotic therapy was stopped, and PD was temporarily suspended. Systemic and effluent markers of inflammation took 4 weeks to normalize. The patient did not regain his usual state of health until several weeks after discharge. Follow-up CT scan showed considerable pancreatic sequelae.</p><p><strong>Conclusion: </strong>Acute pancreatitis is an important cause of PD peritonitis. Negative dialysate cultures and unsatisfactory clinical response should trigger evaluation for acute pancreatitis and its multiple potential causes, including PD treatment itself. Serum lipase levels >3 times ULN and elevated dialysis fluid lipase can be expected. Timely performance of imaging is advisable. Prognosis can be poor, and close monitoring is recommended.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"14 1","pages":"70-80"},"PeriodicalIF":0.9000,"publicationDate":"2024-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11250623/pdf/","citationCount":"0","resultStr":"{\"title\":\"Peritonitis in Peritoneal Dialysis: When to Consider Acute Pancreatitis? Case Report and Mini-Review.\",\"authors\":\"Simeon Schietzel, Sarah Jane Rippin Wagner, Luzia Nigg Calanca\",\"doi\":\"10.1159/000539185\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Acute pancreatitis is an infrequent but challenging cause of peritonitis in peritoneal dialysis (PD). Presentation is often indistinguishable from infectious peritonitis, interpretation of pancreatic enzymes is not straight-forward, and multiple etiologies need to be considered.</p><p><strong>Case presentation: </strong>A 74-year-old PD patient presented with cloudy dialysate and subtle symptoms of malaise and abdominal pain. WBC was 26,000/µL, CRP was 250 mg/L, and dialysis effluent contained 1,047 leucocytes/μL (90% polymorphs). Infectious peritonitis was presumed, and antibiotic treatment started. However, dialysate cultures remained negative, effluent leucocyte count remained high, and clinical condition deteriorated. Abdominal ultrasound was unremarkable (pancreas not visible). Acute pancreatitis was diagnosed by elevated lipase level (serum: 628 U/L, dialysis fluid: 15 U/L) and CT scan. Disentangling etiological factors was challenging. The patient had gallstones, consumed alcoholic beverages, was recently on doxycycline and dialyzed with icodextrin. In addition, PD treatment itself may have been a contributory factor. Antibiotic therapy was stopped, and PD was temporarily suspended. Systemic and effluent markers of inflammation took 4 weeks to normalize. The patient did not regain his usual state of health until several weeks after discharge. Follow-up CT scan showed considerable pancreatic sequelae.</p><p><strong>Conclusion: </strong>Acute pancreatitis is an important cause of PD peritonitis. Negative dialysate cultures and unsatisfactory clinical response should trigger evaluation for acute pancreatitis and its multiple potential causes, including PD treatment itself. Serum lipase levels >3 times ULN and elevated dialysis fluid lipase can be expected. Timely performance of imaging is advisable. Prognosis can be poor, and close monitoring is recommended.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"14 1\",\"pages\":\"70-80\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-06-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11250623/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000539185\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000539185","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Peritonitis in Peritoneal Dialysis: When to Consider Acute Pancreatitis? Case Report and Mini-Review.
Introduction: Acute pancreatitis is an infrequent but challenging cause of peritonitis in peritoneal dialysis (PD). Presentation is often indistinguishable from infectious peritonitis, interpretation of pancreatic enzymes is not straight-forward, and multiple etiologies need to be considered.
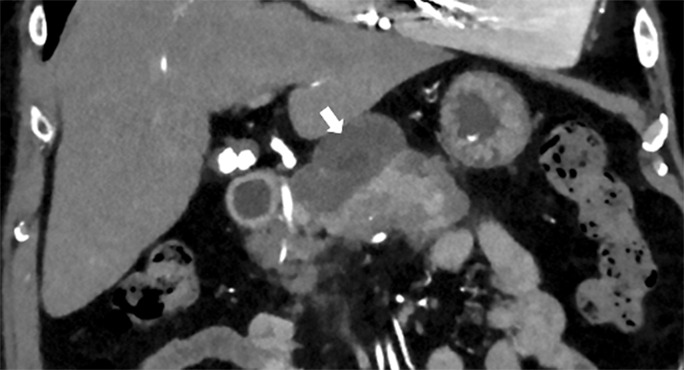
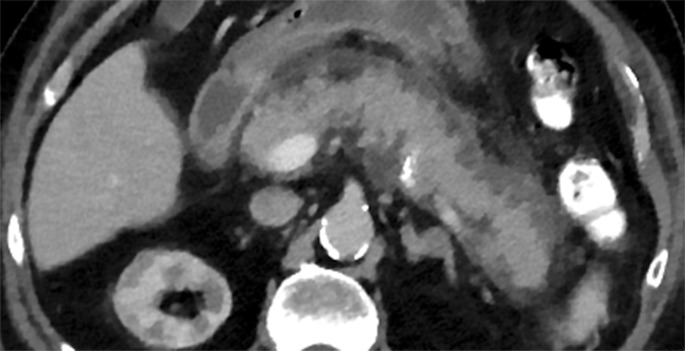
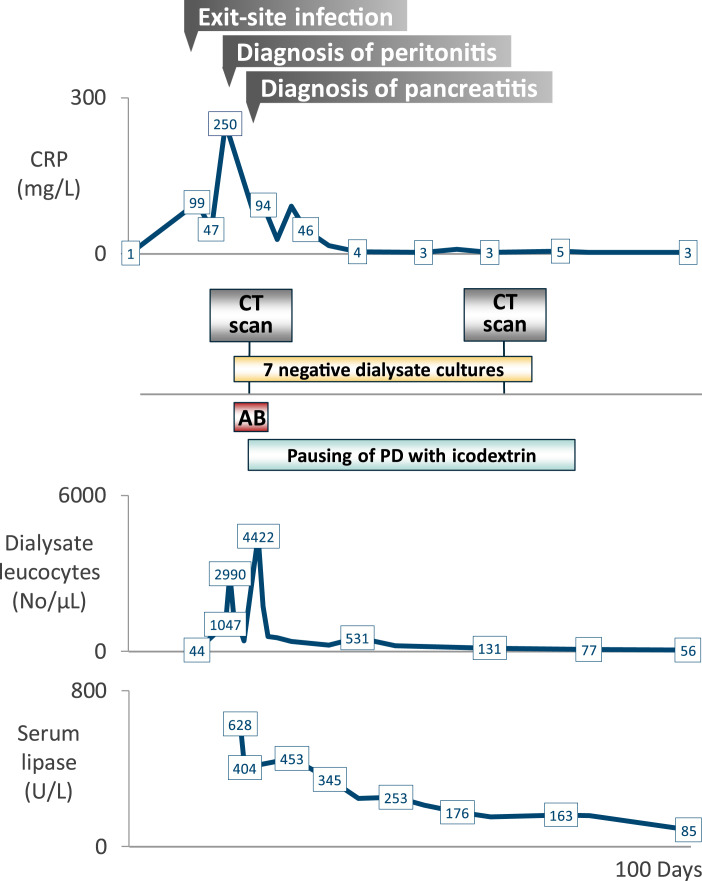
Case presentation: A 74-year-old PD patient presented with cloudy dialysate and subtle symptoms of malaise and abdominal pain. WBC was 26,000/µL, CRP was 250 mg/L, and dialysis effluent contained 1,047 leucocytes/μL (90% polymorphs). Infectious peritonitis was presumed, and antibiotic treatment started. However, dialysate cultures remained negative, effluent leucocyte count remained high, and clinical condition deteriorated. Abdominal ultrasound was unremarkable (pancreas not visible). Acute pancreatitis was diagnosed by elevated lipase level (serum: 628 U/L, dialysis fluid: 15 U/L) and CT scan. Disentangling etiological factors was challenging. The patient had gallstones, consumed alcoholic beverages, was recently on doxycycline and dialyzed with icodextrin. In addition, PD treatment itself may have been a contributory factor. Antibiotic therapy was stopped, and PD was temporarily suspended. Systemic and effluent markers of inflammation took 4 weeks to normalize. The patient did not regain his usual state of health until several weeks after discharge. Follow-up CT scan showed considerable pancreatic sequelae.
Conclusion: Acute pancreatitis is an important cause of PD peritonitis. Negative dialysate cultures and unsatisfactory clinical response should trigger evaluation for acute pancreatitis and its multiple potential causes, including PD treatment itself. Serum lipase levels >3 times ULN and elevated dialysis fluid lipase can be expected. Timely performance of imaging is advisable. Prognosis can be poor, and close monitoring is recommended.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


