Jung Yin Tsang, Matthew Sperrin, Thomas Blakeman, Rupert A Payne, Darren M Ashcroft
{"title":"多药疗法评估评分的开发和验证规程。","authors":"Jung Yin Tsang, Matthew Sperrin, Thomas Blakeman, Rupert A Payne, Darren M Ashcroft","doi":"10.1186/s41512-024-00171-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An increasing number of people are using multiple medications each day, named polypharmacy. This is driven by an ageing population, increasing multimorbidity, and single disease-focussed guidelines. Medications carry obvious benefits, yet polypharmacy is also linked to adverse consequences including adverse drug events, drug-drug and drug-disease interactions, poor patient experience and wasted resources. Problematic polypharmacy is 'the prescribing of multiple medicines inappropriately, or where the intended benefits are not realised'. Identifying people with problematic polypharmacy is complex, as multiple medicines can be suitable for people with several chronic conditions requiring more treatment. Hence, polypharmacy is often potentially problematic, rather than always inappropriate, dependent on clinical context and individual benefit vs risk. There is a need to improve how we identify and evaluate these patients by extending beyond simple counts of medicines to include individual factors and long-term conditions.</p><p><strong>Aim: </strong>To produce a Polypharmacy Assessment Score to identify a population with unusual levels of prescribing who may be at risk of potentially problematic polypharmacy.</p><p><strong>Methods: </strong>Analyses will be performed in three parts: 1. A prediction model will be constructed using observed medications count as the dependent variable, with age, gender and long-term conditions as independent variables. A 'Polypharmacy Assessment Score' will then be constructed through calculating the differences between the observed and expected count of prescribed medications, thereby highlighting people that have unexpected levels of prescribing. Parts 2 and 3 will examine different aspects of validity of the Polypharmacy Assessment Score: 2. To assess 'construct validity', cross-sectional analyses will evaluate high-risk prescribing within populations defined by a range of Polypharmacy Assessment Scores, using both explicit (STOPP/START criteria) and implicit (Medication Appropriateness Index) measures of inappropriate prescribing. 3. To assess 'predictive validity', a retrospective cohort study will explore differences in clinical outcomes (adverse drug reactions, unplanned hospitalisation and all-cause mortality) between differing scores.</p><p><strong>Discussion: </strong>Developing a cross-cutting measure of polypharmacy may allow healthcare professionals to prioritise and risk stratify patients with polypharmacy using unusual levels of prescribing. This would be an improvement from current approaches of either using simple cutoffs or narrow prescribing criteria.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"8 1","pages":"10"},"PeriodicalIF":2.6000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11251249/pdf/","citationCount":"0","resultStr":"{\"title\":\"Protocol for the development and validation of a Polypharmacy Assessment Score.\",\"authors\":\"Jung Yin Tsang, Matthew Sperrin, Thomas Blakeman, Rupert A Payne, Darren M Ashcroft\",\"doi\":\"10.1186/s41512-024-00171-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>An increasing number of people are using multiple medications each day, named polypharmacy. This is driven by an ageing population, increasing multimorbidity, and single disease-focussed guidelines. Medications carry obvious benefits, yet polypharmacy is also linked to adverse consequences including adverse drug events, drug-drug and drug-disease interactions, poor patient experience and wasted resources. Problematic polypharmacy is 'the prescribing of multiple medicines inappropriately, or where the intended benefits are not realised'. Identifying people with problematic polypharmacy is complex, as multiple medicines can be suitable for people with several chronic conditions requiring more treatment. Hence, polypharmacy is often potentially problematic, rather than always inappropriate, dependent on clinical context and individual benefit vs risk. There is a need to improve how we identify and evaluate these patients by extending beyond simple counts of medicines to include individual factors and long-term conditions.</p><p><strong>Aim: </strong>To produce a Polypharmacy Assessment Score to identify a population with unusual levels of prescribing who may be at risk of potentially problematic polypharmacy.</p><p><strong>Methods: </strong>Analyses will be performed in three parts: 1. A prediction model will be constructed using observed medications count as the dependent variable, with age, gender and long-term conditions as independent variables. A 'Polypharmacy Assessment Score' will then be constructed through calculating the differences between the observed and expected count of prescribed medications, thereby highlighting people that have unexpected levels of prescribing. Parts 2 and 3 will examine different aspects of validity of the Polypharmacy Assessment Score: 2. To assess 'construct validity', cross-sectional analyses will evaluate high-risk prescribing within populations defined by a range of Polypharmacy Assessment Scores, using both explicit (STOPP/START criteria) and implicit (Medication Appropriateness Index) measures of inappropriate prescribing. 3. To assess 'predictive validity', a retrospective cohort study will explore differences in clinical outcomes (adverse drug reactions, unplanned hospitalisation and all-cause mortality) between differing scores.</p><p><strong>Discussion: </strong>Developing a cross-cutting measure of polypharmacy may allow healthcare professionals to prioritise and risk stratify patients with polypharmacy using unusual levels of prescribing. This would be an improvement from current approaches of either using simple cutoffs or narrow prescribing criteria.</p>\",\"PeriodicalId\":72800,\"journal\":{\"name\":\"Diagnostic and prognostic research\",\"volume\":\"8 1\",\"pages\":\"10\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11251249/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diagnostic and prognostic research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41512-024-00171-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-024-00171-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Protocol for the development and validation of a Polypharmacy Assessment Score.
Background: An increasing number of people are using multiple medications each day, named polypharmacy. This is driven by an ageing population, increasing multimorbidity, and single disease-focussed guidelines. Medications carry obvious benefits, yet polypharmacy is also linked to adverse consequences including adverse drug events, drug-drug and drug-disease interactions, poor patient experience and wasted resources. Problematic polypharmacy is 'the prescribing of multiple medicines inappropriately, or where the intended benefits are not realised'. Identifying people with problematic polypharmacy is complex, as multiple medicines can be suitable for people with several chronic conditions requiring more treatment. Hence, polypharmacy is often potentially problematic, rather than always inappropriate, dependent on clinical context and individual benefit vs risk. There is a need to improve how we identify and evaluate these patients by extending beyond simple counts of medicines to include individual factors and long-term conditions.
Aim: To produce a Polypharmacy Assessment Score to identify a population with unusual levels of prescribing who may be at risk of potentially problematic polypharmacy.
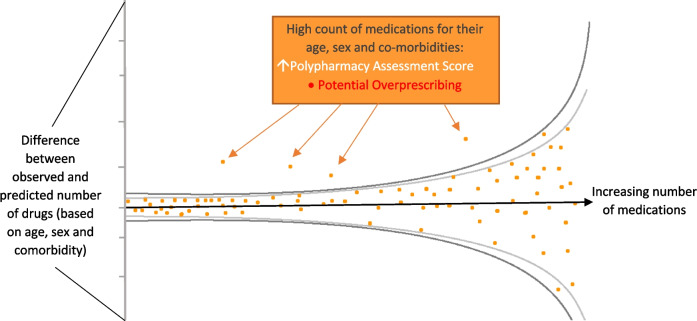
Methods: Analyses will be performed in three parts: 1. A prediction model will be constructed using observed medications count as the dependent variable, with age, gender and long-term conditions as independent variables. A 'Polypharmacy Assessment Score' will then be constructed through calculating the differences between the observed and expected count of prescribed medications, thereby highlighting people that have unexpected levels of prescribing. Parts 2 and 3 will examine different aspects of validity of the Polypharmacy Assessment Score: 2. To assess 'construct validity', cross-sectional analyses will evaluate high-risk prescribing within populations defined by a range of Polypharmacy Assessment Scores, using both explicit (STOPP/START criteria) and implicit (Medication Appropriateness Index) measures of inappropriate prescribing. 3. To assess 'predictive validity', a retrospective cohort study will explore differences in clinical outcomes (adverse drug reactions, unplanned hospitalisation and all-cause mortality) between differing scores.
Discussion: Developing a cross-cutting measure of polypharmacy may allow healthcare professionals to prioritise and risk stratify patients with polypharmacy using unusual levels of prescribing. This would be an improvement from current approaches of either using simple cutoffs or narrow prescribing criteria.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


