Geoffrey Z. L. Kuppens, Kathelijn Fischer, Karin P. M. van Galen, Eduard J. van Beers, Paul R. Van der Valk, Idske C. L. Kremer Hovinga, Lize F. D. van Vulpen, Roger E. G. Schutgens
{"title":"1:1比例的VWF/FVIII浓缩液对von Willebrand病患者的疗效。","authors":"Geoffrey Z. L. Kuppens, Kathelijn Fischer, Karin P. M. van Galen, Eduard J. van Beers, Paul R. Van der Valk, Idske C. L. Kremer Hovinga, Lize F. D. van Vulpen, Roger E. G. Schutgens","doi":"10.1111/hae.15079","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Patients with von Willebrand disease (VWD) require administration of von Willebrand factor (VWF) concentrates peri-operatively. Concerns about FVIII accumulation after repetitive injections of a 1:1 ratio VWF/FVIII clotting factor concentrate (CFC) led this study to explore the recovery and FVIII accumulation over time.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This monocentre study examined patients with VWD receiving perioperative 1:1 ratio CFC infusions. CFC dosing was based on body weight and endogenous VWF/FVIII activity. FVIII and VWF activity was monitored at T0 (baseline), T1 (15 min postinfusion), and trough levels at T2-T6 (24-120 h).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We included 125 patients, undergoing 125 procedures (63 major surgeries, 62 minor), with a median of two CFC infusions (IQR 1–3). With a mean administered dose of 35.7 IU/kg CFC, recovery rates of FVIII and VWF were 2.6 IU/dL per IU/kg and 2.4 IU/dL per IU/kg, respectively. Mean FVIII levels at T0 were 62 (SD 51.9), T1: 164 (SD 80.4), T2: 155 (SD 62.8), T3: 162 (SD 59.8), T4: 124 (SD 78.4), and T5: 120 (SD 65.3) IU/dL. Mean VWF activity levels at T0 were 29 (SD 25.0), T1: 133 (SD 43.7), T2: 92 (SD 37.2), and T3: 86 (SD 37.5) IU/dL. Subgroup analysis in 47 patients with more than three infusions, showed no accumulation of mean FVIII levels.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This perioperative study demonstrated excellent FVIII and VWF recovery of a 1:1 ratio VWF product in patients with VWD. Stable FVIII and VWF activity levels were observed after repeated infusions, without accumulation. Most major surgeries required only three CFC infusions.</p>\n </section>\n </div>","PeriodicalId":12819,"journal":{"name":"Haemophilia","volume":"30 5","pages":"1148-1154"},"PeriodicalIF":3.0000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.15079","citationCount":"0","resultStr":"{\"title\":\"Efficacy of a 1:1 ratio VWF/FVIII concentrate in patients with von Willebrand disease\",\"authors\":\"Geoffrey Z. L. Kuppens, Kathelijn Fischer, Karin P. M. van Galen, Eduard J. van Beers, Paul R. Van der Valk, Idske C. L. Kremer Hovinga, Lize F. D. van Vulpen, Roger E. G. Schutgens\",\"doi\":\"10.1111/hae.15079\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Patients with von Willebrand disease (VWD) require administration of von Willebrand factor (VWF) concentrates peri-operatively. Concerns about FVIII accumulation after repetitive injections of a 1:1 ratio VWF/FVIII clotting factor concentrate (CFC) led this study to explore the recovery and FVIII accumulation over time.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This monocentre study examined patients with VWD receiving perioperative 1:1 ratio CFC infusions. CFC dosing was based on body weight and endogenous VWF/FVIII activity. FVIII and VWF activity was monitored at T0 (baseline), T1 (15 min postinfusion), and trough levels at T2-T6 (24-120 h).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We included 125 patients, undergoing 125 procedures (63 major surgeries, 62 minor), with a median of two CFC infusions (IQR 1–3). With a mean administered dose of 35.7 IU/kg CFC, recovery rates of FVIII and VWF were 2.6 IU/dL per IU/kg and 2.4 IU/dL per IU/kg, respectively. Mean FVIII levels at T0 were 62 (SD 51.9), T1: 164 (SD 80.4), T2: 155 (SD 62.8), T3: 162 (SD 59.8), T4: 124 (SD 78.4), and T5: 120 (SD 65.3) IU/dL. Mean VWF activity levels at T0 were 29 (SD 25.0), T1: 133 (SD 43.7), T2: 92 (SD 37.2), and T3: 86 (SD 37.5) IU/dL. Subgroup analysis in 47 patients with more than three infusions, showed no accumulation of mean FVIII levels.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>This perioperative study demonstrated excellent FVIII and VWF recovery of a 1:1 ratio VWF product in patients with VWD. Stable FVIII and VWF activity levels were observed after repeated infusions, without accumulation. Most major surgeries required only three CFC infusions.</p>\\n </section>\\n </div>\",\"PeriodicalId\":12819,\"journal\":{\"name\":\"Haemophilia\",\"volume\":\"30 5\",\"pages\":\"1148-1154\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.15079\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Haemophilia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/hae.15079\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Haemophilia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hae.15079","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Efficacy of a 1:1 ratio VWF/FVIII concentrate in patients with von Willebrand disease
Introduction
Patients with von Willebrand disease (VWD) require administration of von Willebrand factor (VWF) concentrates peri-operatively. Concerns about FVIII accumulation after repetitive injections of a 1:1 ratio VWF/FVIII clotting factor concentrate (CFC) led this study to explore the recovery and FVIII accumulation over time.
Methods
This monocentre study examined patients with VWD receiving perioperative 1:1 ratio CFC infusions. CFC dosing was based on body weight and endogenous VWF/FVIII activity. FVIII and VWF activity was monitored at T0 (baseline), T1 (15 min postinfusion), and trough levels at T2-T6 (24-120 h).
Results
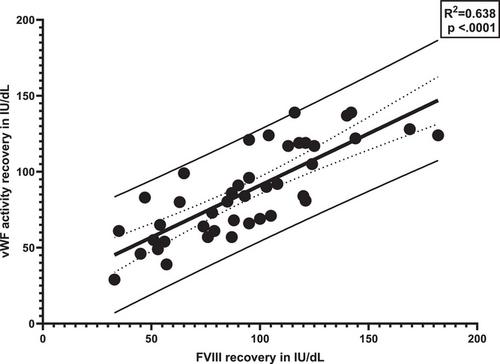
We included 125 patients, undergoing 125 procedures (63 major surgeries, 62 minor), with a median of two CFC infusions (IQR 1–3). With a mean administered dose of 35.7 IU/kg CFC, recovery rates of FVIII and VWF were 2.6 IU/dL per IU/kg and 2.4 IU/dL per IU/kg, respectively. Mean FVIII levels at T0 were 62 (SD 51.9), T1: 164 (SD 80.4), T2: 155 (SD 62.8), T3: 162 (SD 59.8), T4: 124 (SD 78.4), and T5: 120 (SD 65.3) IU/dL. Mean VWF activity levels at T0 were 29 (SD 25.0), T1: 133 (SD 43.7), T2: 92 (SD 37.2), and T3: 86 (SD 37.5) IU/dL. Subgroup analysis in 47 patients with more than three infusions, showed no accumulation of mean FVIII levels.
Conclusion
This perioperative study demonstrated excellent FVIII and VWF recovery of a 1:1 ratio VWF product in patients with VWD. Stable FVIII and VWF activity levels were observed after repeated infusions, without accumulation. Most major surgeries required only three CFC infusions.
期刊介绍:
Haemophilia is an international journal dedicated to the exchange of information regarding the comprehensive care of haemophilia. The Journal contains review articles, original scientific papers and case reports related to haemophilia care, with frequent supplements. Subjects covered include:
clotting factor deficiencies, both inherited and acquired: haemophilia A, B, von Willebrand''s disease, deficiencies of factor V, VII, X and XI
replacement therapy for clotting factor deficiencies
component therapy in the developing world
transfusion transmitted disease
haemophilia care and paediatrics, orthopaedics, gynaecology and obstetrics
nursing
laboratory diagnosis
carrier detection
psycho-social concerns
economic issues
audit
inherited platelet disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


