Nicole Russell, Ethan J Vieira, Lexi R Freeman, Alexander L Eastman, Uzer Khan, Haley M Schluterman, Caroline Beakes, Sioned Kirkpatrick, Jennifer L Grant
{"title":"平民血管内弹道栓塞病例的诊断和治疗注意事项:病例报告综述。","authors":"Nicole Russell, Ethan J Vieira, Lexi R Freeman, Alexander L Eastman, Uzer Khan, Haley M Schluterman, Caroline Beakes, Sioned Kirkpatrick, Jennifer L Grant","doi":"10.1136/tsaco-2024-001390","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ballistic embolism (BE) is a rare complication of firearm injuries notoriously associated with a vexing clinical picture in the trauma bay. Unless considered early, the associated confusion can lead to needless delay in the management of the patient with a gunshot wound. Despite this known entity, there is a relative paucity of high-grade evidence regarding complications, management, and follow-up in these patients.</p><p><strong>Methods: </strong>An electronic database literature search was conducted to identify cases of acute intravascular BE in pediatric and adult civilians occurring during index hospitalization, filtered to publications during the past 10 years. Exclusion criteria included non-vascular embolization, injuries occurring in the military setting, and delayed migration defined as occurring after discharge from the index hospitalization.</p><p><strong>Results: </strong>A total of 136 cases were analyzed. Nearly all cases of BE occurred within 48 hours of presentation. Compared with venous emboli, arterial emboli were significantly more likely to be symptomatic (71% vs. 7%, p<0.001), and 43% of patients developed symptoms attributable to BE in the trauma bay. In addition, arterial emboli were significantly less likely to be managed non-invasively (19% vs. 49%, p<0.001). Open retrieval was significantly more likely to be successful compared with endovascular attempts (91% vs. 29%, p<0.001). Patients with arterial emboli were more likely to receive follow-up (52% vs. 39%) and any attempt at retrieval during the hospitalization was significantly associated with outpatient follow-up (p=0.034). All but one patient remained stable or had clinically improved symptoms after discharge.</p><p><strong>Conclusion: </strong>Consideration for BE is reasonable in any patient with new or persistent unexplained signs or symptoms, especially during the first 48 hours after a penetrating firearm injury. Although venous BE can often be safely observed, arterial BE generally necessitates urgent retrieval. Patients who are managed non-invasively may benefit from follow-up in the first year after injury.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"9 1","pages":"e001390"},"PeriodicalIF":2.2000,"publicationDate":"2024-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11243208/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic and therapeutic considerations in cases of civilian intravascular ballistic embolism: a review of case reports.\",\"authors\":\"Nicole Russell, Ethan J Vieira, Lexi R Freeman, Alexander L Eastman, Uzer Khan, Haley M Schluterman, Caroline Beakes, Sioned Kirkpatrick, Jennifer L Grant\",\"doi\":\"10.1136/tsaco-2024-001390\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ballistic embolism (BE) is a rare complication of firearm injuries notoriously associated with a vexing clinical picture in the trauma bay. Unless considered early, the associated confusion can lead to needless delay in the management of the patient with a gunshot wound. Despite this known entity, there is a relative paucity of high-grade evidence regarding complications, management, and follow-up in these patients.</p><p><strong>Methods: </strong>An electronic database literature search was conducted to identify cases of acute intravascular BE in pediatric and adult civilians occurring during index hospitalization, filtered to publications during the past 10 years. Exclusion criteria included non-vascular embolization, injuries occurring in the military setting, and delayed migration defined as occurring after discharge from the index hospitalization.</p><p><strong>Results: </strong>A total of 136 cases were analyzed. Nearly all cases of BE occurred within 48 hours of presentation. Compared with venous emboli, arterial emboli were significantly more likely to be symptomatic (71% vs. 7%, p<0.001), and 43% of patients developed symptoms attributable to BE in the trauma bay. In addition, arterial emboli were significantly less likely to be managed non-invasively (19% vs. 49%, p<0.001). Open retrieval was significantly more likely to be successful compared with endovascular attempts (91% vs. 29%, p<0.001). Patients with arterial emboli were more likely to receive follow-up (52% vs. 39%) and any attempt at retrieval during the hospitalization was significantly associated with outpatient follow-up (p=0.034). All but one patient remained stable or had clinically improved symptoms after discharge.</p><p><strong>Conclusion: </strong>Consideration for BE is reasonable in any patient with new or persistent unexplained signs or symptoms, especially during the first 48 hours after a penetrating firearm injury. Although venous BE can often be safely observed, arterial BE generally necessitates urgent retrieval. Patients who are managed non-invasively may benefit from follow-up in the first year after injury.</p>\",\"PeriodicalId\":23307,\"journal\":{\"name\":\"Trauma Surgery & Acute Care Open\",\"volume\":\"9 1\",\"pages\":\"e001390\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-07-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11243208/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Trauma Surgery & Acute Care Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/tsaco-2024-001390\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001390","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:弹道栓塞(BE)是一种罕见的枪伤并发症,在外伤室的临床表现令人头疼。除非及早考虑,否则相关的混淆会导致枪伤患者的治疗出现不必要的延误。尽管这种情况众所周知,但有关这些患者的并发症、治疗和随访的高级证据却相对匮乏:方法:通过电子数据库文献检索,筛选出过去 10 年内发表的、发生在儿童和成人住院期间的急性血管内 BE 病例。排除标准包括非血管性栓塞、发生在军事环境中的伤害以及延迟迁移,延迟迁移的定义是发生在急诊出院后:结果:共分析了 136 个病例。几乎所有的BE病例都发生在发病后48小时内。与静脉栓塞相比,动脉栓塞出现症状的几率明显更高(71% 对 7%,P):对于任何有新的或持续的不明体征或症状的患者,尤其是在穿透性火器伤害后的 48 小时内,考虑 BE 是合理的。虽然静脉 BE 通常可以安全观察,但动脉 BE 通常需要紧急取出。无创治疗的患者可能会受益于伤后第一年的随访。
Diagnostic and therapeutic considerations in cases of civilian intravascular ballistic embolism: a review of case reports.
Background: Ballistic embolism (BE) is a rare complication of firearm injuries notoriously associated with a vexing clinical picture in the trauma bay. Unless considered early, the associated confusion can lead to needless delay in the management of the patient with a gunshot wound. Despite this known entity, there is a relative paucity of high-grade evidence regarding complications, management, and follow-up in these patients.
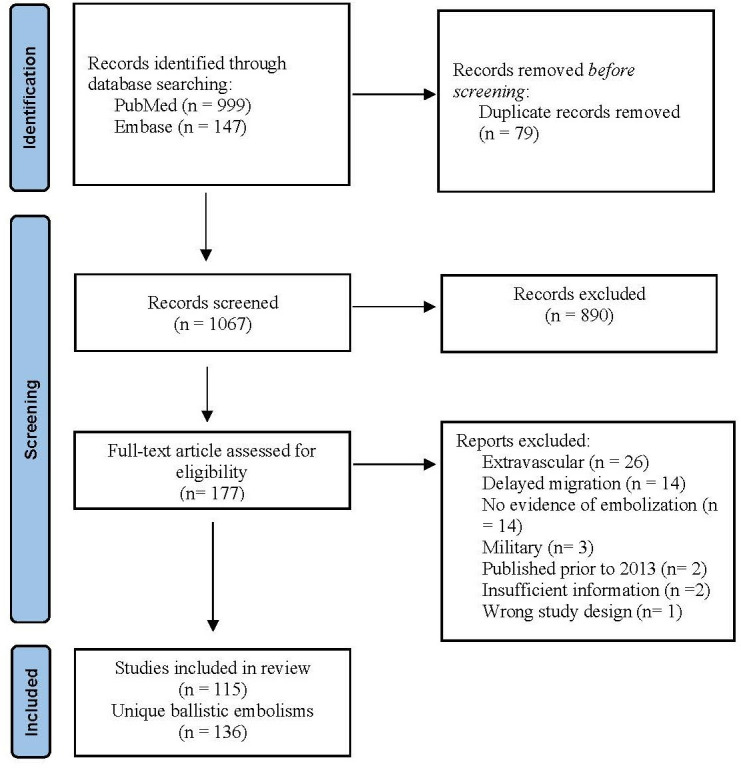
Methods: An electronic database literature search was conducted to identify cases of acute intravascular BE in pediatric and adult civilians occurring during index hospitalization, filtered to publications during the past 10 years. Exclusion criteria included non-vascular embolization, injuries occurring in the military setting, and delayed migration defined as occurring after discharge from the index hospitalization.
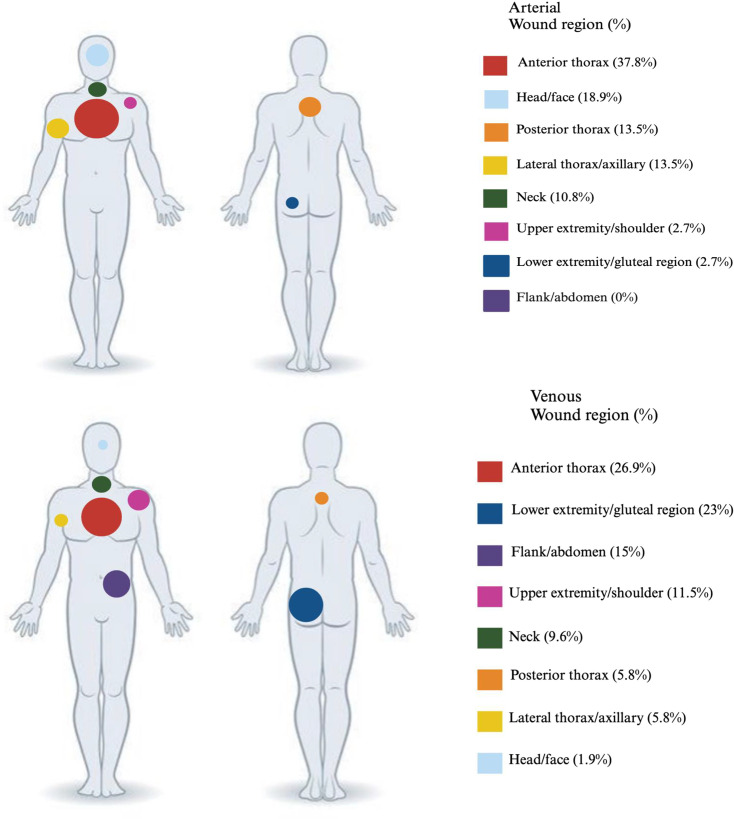
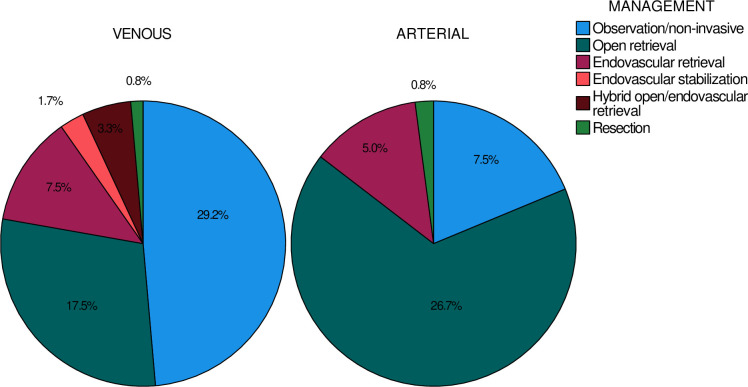
Results: A total of 136 cases were analyzed. Nearly all cases of BE occurred within 48 hours of presentation. Compared with venous emboli, arterial emboli were significantly more likely to be symptomatic (71% vs. 7%, p<0.001), and 43% of patients developed symptoms attributable to BE in the trauma bay. In addition, arterial emboli were significantly less likely to be managed non-invasively (19% vs. 49%, p<0.001). Open retrieval was significantly more likely to be successful compared with endovascular attempts (91% vs. 29%, p<0.001). Patients with arterial emboli were more likely to receive follow-up (52% vs. 39%) and any attempt at retrieval during the hospitalization was significantly associated with outpatient follow-up (p=0.034). All but one patient remained stable or had clinically improved symptoms after discharge.
Conclusion: Consideration for BE is reasonable in any patient with new or persistent unexplained signs or symptoms, especially during the first 48 hours after a penetrating firearm injury. Although venous BE can often be safely observed, arterial BE generally necessitates urgent retrieval. Patients who are managed non-invasively may benefit from follow-up in the first year after injury.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


