Ingrid Toews, Salman Hussain, John L Z Nyirenda, Maria A Willis, Lucia Kantorová, Simona Slezáková, Minyahil Tadesse Boltena, John Victor Peter, Luis Eduardo Santos Fontes, Miloslav Klugar, Behnam Sadeghirad, Joerg J Meerpohl
{"title":"预防重症监护室住院患者上消化道出血的药物干预:网络荟萃分析。","authors":"Ingrid Toews, Salman Hussain, John L Z Nyirenda, Maria A Willis, Lucia Kantorová, Simona Slezáková, Minyahil Tadesse Boltena, John Victor Peter, Luis Eduardo Santos Fontes, Miloslav Klugar, Behnam Sadeghirad, Joerg J Meerpohl","doi":"10.1136/bmjebm-2024-112886","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the efficacy and safety of pharmacological interventions for preventing upper gastrointestinal (GI) bleeding in people admitted to intensive care units (ICUs).</p><p><strong>Design and setting: </strong>Systematic review and frequentist network meta-analysis using standard methodological procedures as recommended by Cochrane for screening of records, data extraction and analysis. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence.</p><p><strong>Participants: </strong>Randomised controlled trials involving patients admitted to ICUs for longer than 24 hours were included.</p><p><strong>Search methods: </strong>The Cochrane Gut Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase and Latin American and Caribbean Health Science Information database (LILACS) databases were searched from August 2017 to March 2022. The search in MEDLINE was updated in April 2023. We also searched ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP).</p><p><strong>Main outcome measures: </strong>The primary outcome was the prevention of clinically important upper GI bleeding.</p><p><strong>Results: </strong>We included 123 studies with 46 996 participants. Cimetidine (relative risk (RR) 0.56, 95% CI 0.40 to 0.77, moderate certainty), ranitidine (RR 0.54, 95% CI 0.38 to 0.76, moderate certainty), antacids (RR 0.48, 95% CI 0.33 to 0.68, moderate certainty), sucralfate (RR 0.54, 95% CI 0.39 to 0.75, moderate certainty) and a combination of ranitidine and antacids (RR 0.13, 95% CI 0.03 to 0.62, moderate certainty) are likely effective in preventing upper GI bleeding.The effect of any intervention on the prevention of nosocomial pneumonia, all-cause mortality in the ICU or the hospital, duration of the stay in the ICU, duration of intubation and (serious) adverse events remains unclear.</p><p><strong>Conclusions: </strong>Several interventions seem effective in preventing clinically important upper GI bleeding while there is limited evidence for other outcomes. Patient-relevant benefits and harms need to be assessed under consideration of the patients' underlying conditions.</p>","PeriodicalId":9059,"journal":{"name":"BMJ Evidence-Based Medicine","volume":" ","pages":"22-35"},"PeriodicalIF":7.6000,"publicationDate":"2025-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11874471/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pharmacological interventions for preventing upper gastrointestinal bleeding in people admitted to intensive care units: a network meta-analysis.\",\"authors\":\"Ingrid Toews, Salman Hussain, John L Z Nyirenda, Maria A Willis, Lucia Kantorová, Simona Slezáková, Minyahil Tadesse Boltena, John Victor Peter, Luis Eduardo Santos Fontes, Miloslav Klugar, Behnam Sadeghirad, Joerg J Meerpohl\",\"doi\":\"10.1136/bmjebm-2024-112886\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess the efficacy and safety of pharmacological interventions for preventing upper gastrointestinal (GI) bleeding in people admitted to intensive care units (ICUs).</p><p><strong>Design and setting: </strong>Systematic review and frequentist network meta-analysis using standard methodological procedures as recommended by Cochrane for screening of records, data extraction and analysis. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence.</p><p><strong>Participants: </strong>Randomised controlled trials involving patients admitted to ICUs for longer than 24 hours were included.</p><p><strong>Search methods: </strong>The Cochrane Gut Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase and Latin American and Caribbean Health Science Information database (LILACS) databases were searched from August 2017 to March 2022. The search in MEDLINE was updated in April 2023. We also searched ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP).</p><p><strong>Main outcome measures: </strong>The primary outcome was the prevention of clinically important upper GI bleeding.</p><p><strong>Results: </strong>We included 123 studies with 46 996 participants. Cimetidine (relative risk (RR) 0.56, 95% CI 0.40 to 0.77, moderate certainty), ranitidine (RR 0.54, 95% CI 0.38 to 0.76, moderate certainty), antacids (RR 0.48, 95% CI 0.33 to 0.68, moderate certainty), sucralfate (RR 0.54, 95% CI 0.39 to 0.75, moderate certainty) and a combination of ranitidine and antacids (RR 0.13, 95% CI 0.03 to 0.62, moderate certainty) are likely effective in preventing upper GI bleeding.The effect of any intervention on the prevention of nosocomial pneumonia, all-cause mortality in the ICU or the hospital, duration of the stay in the ICU, duration of intubation and (serious) adverse events remains unclear.</p><p><strong>Conclusions: </strong>Several interventions seem effective in preventing clinically important upper GI bleeding while there is limited evidence for other outcomes. Patient-relevant benefits and harms need to be assessed under consideration of the patients' underlying conditions.</p>\",\"PeriodicalId\":9059,\"journal\":{\"name\":\"BMJ Evidence-Based Medicine\",\"volume\":\" \",\"pages\":\"22-35\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2025-01-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11874471/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Evidence-Based Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjebm-2024-112886\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Evidence-Based Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjebm-2024-112886","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的评估预防重症监护病房(ICU)住院患者上消化道(GI)出血的药物干预措施的有效性和安全性:系统综述和频数网络荟萃分析,采用 Cochrane 推荐的标准方法筛选记录、提取数据并进行分析。采用建议评估、发展和评价分级法(GRADE)评估证据的确定性:检索方法:从2017年8月到2022年3月,对Cochrane肠道专业注册、Cochrane对照试验中央注册(CENTRAL)、MEDLINE、Embase以及拉丁美洲和加勒比海健康科学信息数据库(LILACS)等数据库进行了检索。MEDLINE的检索于2023年4月更新。我们还检索了ClinicalTrials.gov和世界卫生组织国际临床试验注册平台(WHO ICTRP):主要结果:主要结果是预防临床上重要的上消化道出血:我们纳入了 123 项研究,共有 46 996 名参与者。西米替丁(相对风险 (RR) 0.56,95% CI 0.40 至 0.77,中等确定性)、雷尼替丁(RR 0.54,95% CI 0.38 至 0.76,中等确定性)、抗酸剂(RR 0.48,95% CI 0.33 至 0.68,中等确定性)、琥珀酸盐(RR 0.54,95% CI 0.39 至 0.75,中等确定性)以及雷尼替丁和抗酸剂的组合(RR 0.13,95% CI 0.任何干预措施对预防院内肺炎、重症监护室或医院内全因死亡率、重症监护室住院时间、插管时间和(严重)不良事件的影响仍不明确:结论:一些干预措施似乎能有效预防临床上重要的上消化道出血,但其他结果的证据却很有限。需要根据患者的基本情况评估与患者相关的益处和危害。
Pharmacological interventions for preventing upper gastrointestinal bleeding in people admitted to intensive care units: a network meta-analysis.
Objectives: To assess the efficacy and safety of pharmacological interventions for preventing upper gastrointestinal (GI) bleeding in people admitted to intensive care units (ICUs).
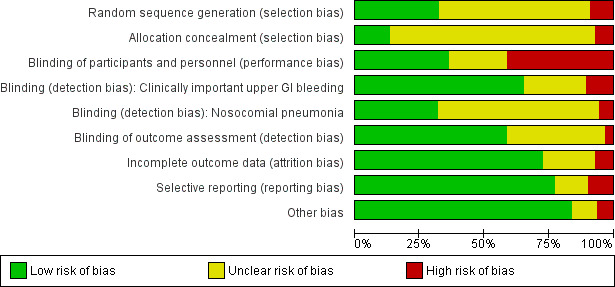
Design and setting: Systematic review and frequentist network meta-analysis using standard methodological procedures as recommended by Cochrane for screening of records, data extraction and analysis. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence.
Participants: Randomised controlled trials involving patients admitted to ICUs for longer than 24 hours were included.
Search methods: The Cochrane Gut Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase and Latin American and Caribbean Health Science Information database (LILACS) databases were searched from August 2017 to March 2022. The search in MEDLINE was updated in April 2023. We also searched ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP).
Main outcome measures: The primary outcome was the prevention of clinically important upper GI bleeding.
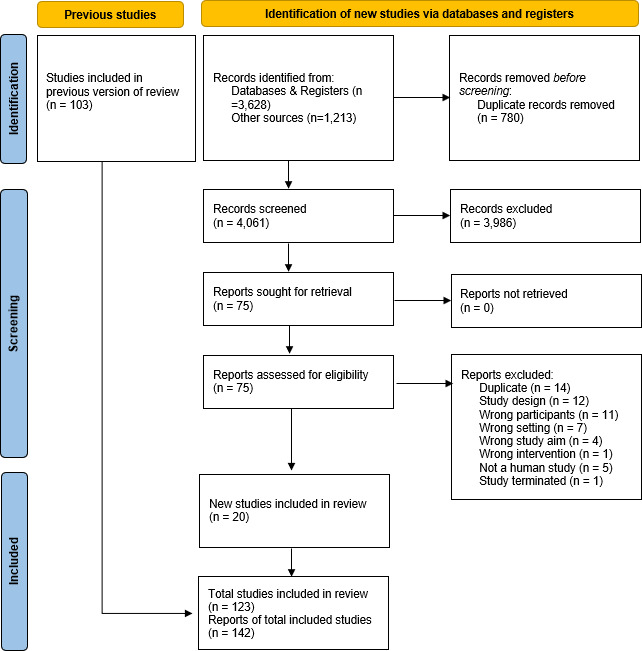
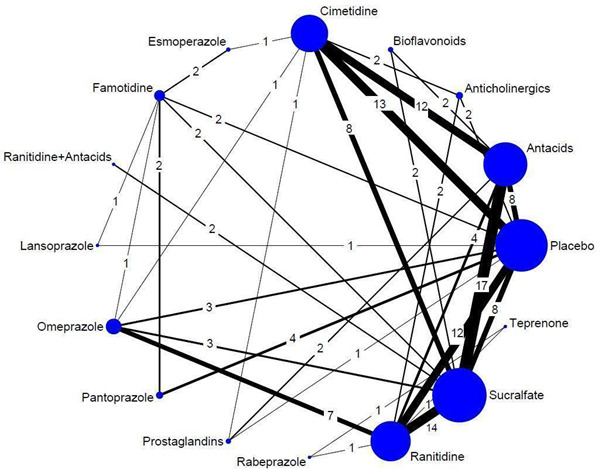
Results: We included 123 studies with 46 996 participants. Cimetidine (relative risk (RR) 0.56, 95% CI 0.40 to 0.77, moderate certainty), ranitidine (RR 0.54, 95% CI 0.38 to 0.76, moderate certainty), antacids (RR 0.48, 95% CI 0.33 to 0.68, moderate certainty), sucralfate (RR 0.54, 95% CI 0.39 to 0.75, moderate certainty) and a combination of ranitidine and antacids (RR 0.13, 95% CI 0.03 to 0.62, moderate certainty) are likely effective in preventing upper GI bleeding.The effect of any intervention on the prevention of nosocomial pneumonia, all-cause mortality in the ICU or the hospital, duration of the stay in the ICU, duration of intubation and (serious) adverse events remains unclear.
Conclusions: Several interventions seem effective in preventing clinically important upper GI bleeding while there is limited evidence for other outcomes. Patient-relevant benefits and harms need to be assessed under consideration of the patients' underlying conditions.
期刊介绍:
BMJ Evidence-Based Medicine (BMJ EBM) publishes original evidence-based research, insights and opinions on what matters for health care. We focus on the tools, methods, and concepts that are basic and central to practising evidence-based medicine and deliver relevant, trustworthy and impactful evidence.
BMJ EBM is a Plan S compliant Transformative Journal and adheres to the highest possible industry standards for editorial policies and publication ethics.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



