Nicolette Centanni, Jennifer Hammond, Joshua Carver, Wendy Craig, Stephanie Nichols
{"title":"细菌感染住院病人静脉注射铁剂:使用情况和结果。","authors":"Nicolette Centanni, Jennifer Hammond, Joshua Carver, Wendy Craig, Stephanie Nichols","doi":"10.46804/2641-2225.1176","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Given the uncertainties related to IV iron therapy and the potential risk of infection, health care providers may hesitate to use this preparation to treat hospitalized patients with bacterial infections, even if clinically indicated. The aim of this study was to examine patterns of prescribing IV iron in patients who were hospitalized and treated for a bacterial infection, and their associated clinical outcomes.</p><p><strong>Methods: </strong>This retrospective chart review evaluated adult patients who received both IV iron sucrose and antibiotics during the same admission at Maine Medical Center in 2019. Data collected included iron studies, practices for prescribing IV iron, and clinical outcomes. Data were summarized using descriptive statistics.</p><p><strong>Results: </strong>A total of 197 patients were evaluated. The median duration of antibiotic therapy was 5(4-9) days. Iron and antibiotic administration overlapped in 153(77.7%) patients, with a mean overlap of 2.7(1-7) days. In the 44 patients without overlap, 20(46%) received IV iron before antibiotics. More than half (57%) of infection types involved urinary tract and respiratory systems. Approximately 2% of patients had antibiotic therapy broadened or duration extended, 7% died, and 16% were readmitted within 30 days of discharge.</p><p><strong>Discussion: </strong>Prior studies evaluating the risk of infection with IV iron published conflicting results. This is the only study that analyzed outcomes in patients receiving IV iron and antibiotics for infection but not undergoing hemodialysis during a hospital admission. Although our findings support that IV iron treatment is safe among patients with concomitant infection and iron deficiency, this finding may not be the case for all clinical subgroups.</p><p><strong>Conclusions: </strong>This study showed that when patients were administered IV iron in the setting of acute bacterial infection in our facility, most patients did not have negative outcomes.</p>","PeriodicalId":93781,"journal":{"name":"Journal of Maine Medical Center","volume":"6 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11238909/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intravenous Iron in Patients Hospitalized with Bacterial Infections: Utilization and Outcomes.\",\"authors\":\"Nicolette Centanni, Jennifer Hammond, Joshua Carver, Wendy Craig, Stephanie Nichols\",\"doi\":\"10.46804/2641-2225.1176\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Given the uncertainties related to IV iron therapy and the potential risk of infection, health care providers may hesitate to use this preparation to treat hospitalized patients with bacterial infections, even if clinically indicated. The aim of this study was to examine patterns of prescribing IV iron in patients who were hospitalized and treated for a bacterial infection, and their associated clinical outcomes.</p><p><strong>Methods: </strong>This retrospective chart review evaluated adult patients who received both IV iron sucrose and antibiotics during the same admission at Maine Medical Center in 2019. Data collected included iron studies, practices for prescribing IV iron, and clinical outcomes. Data were summarized using descriptive statistics.</p><p><strong>Results: </strong>A total of 197 patients were evaluated. The median duration of antibiotic therapy was 5(4-9) days. Iron and antibiotic administration overlapped in 153(77.7%) patients, with a mean overlap of 2.7(1-7) days. In the 44 patients without overlap, 20(46%) received IV iron before antibiotics. More than half (57%) of infection types involved urinary tract and respiratory systems. Approximately 2% of patients had antibiotic therapy broadened or duration extended, 7% died, and 16% were readmitted within 30 days of discharge.</p><p><strong>Discussion: </strong>Prior studies evaluating the risk of infection with IV iron published conflicting results. This is the only study that analyzed outcomes in patients receiving IV iron and antibiotics for infection but not undergoing hemodialysis during a hospital admission. Although our findings support that IV iron treatment is safe among patients with concomitant infection and iron deficiency, this finding may not be the case for all clinical subgroups.</p><p><strong>Conclusions: </strong>This study showed that when patients were administered IV iron in the setting of acute bacterial infection in our facility, most patients did not have negative outcomes.</p>\",\"PeriodicalId\":93781,\"journal\":{\"name\":\"Journal of Maine Medical Center\",\"volume\":\"6 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11238909/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Maine Medical Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.46804/2641-2225.1176\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Maine Medical Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.46804/2641-2225.1176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/18 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Intravenous Iron in Patients Hospitalized with Bacterial Infections: Utilization and Outcomes.
Introduction: Given the uncertainties related to IV iron therapy and the potential risk of infection, health care providers may hesitate to use this preparation to treat hospitalized patients with bacterial infections, even if clinically indicated. The aim of this study was to examine patterns of prescribing IV iron in patients who were hospitalized and treated for a bacterial infection, and their associated clinical outcomes.
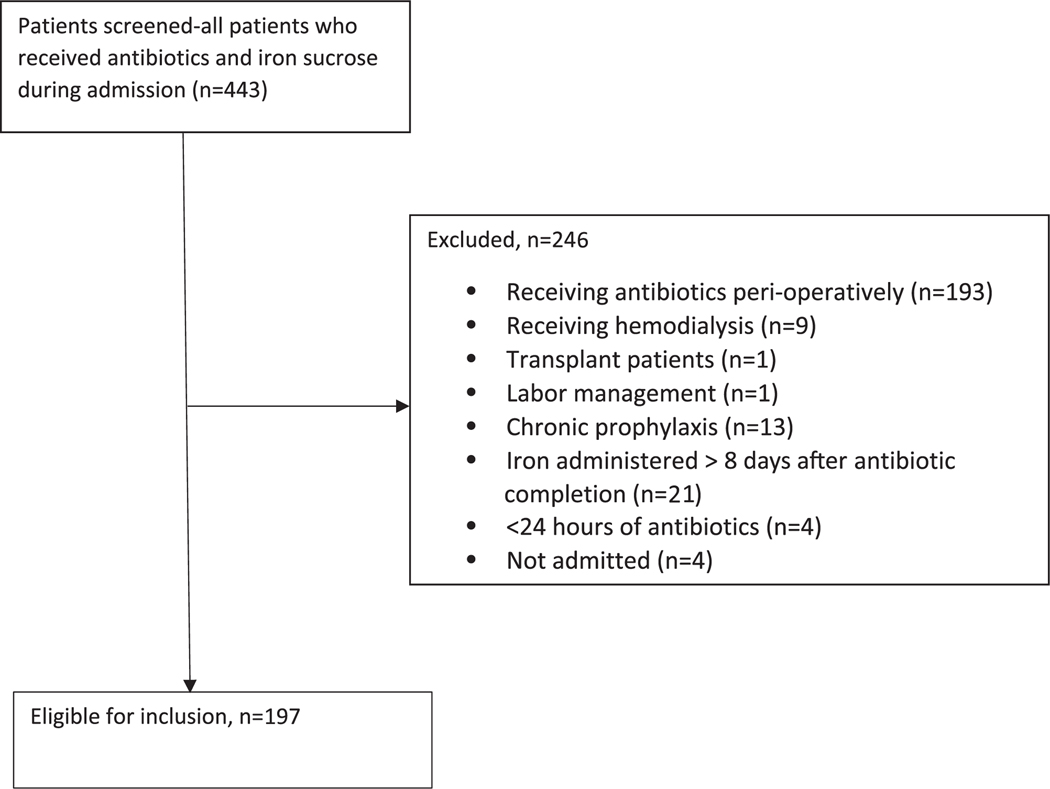
Methods: This retrospective chart review evaluated adult patients who received both IV iron sucrose and antibiotics during the same admission at Maine Medical Center in 2019. Data collected included iron studies, practices for prescribing IV iron, and clinical outcomes. Data were summarized using descriptive statistics.
Results: A total of 197 patients were evaluated. The median duration of antibiotic therapy was 5(4-9) days. Iron and antibiotic administration overlapped in 153(77.7%) patients, with a mean overlap of 2.7(1-7) days. In the 44 patients without overlap, 20(46%) received IV iron before antibiotics. More than half (57%) of infection types involved urinary tract and respiratory systems. Approximately 2% of patients had antibiotic therapy broadened or duration extended, 7% died, and 16% were readmitted within 30 days of discharge.
Discussion: Prior studies evaluating the risk of infection with IV iron published conflicting results. This is the only study that analyzed outcomes in patients receiving IV iron and antibiotics for infection but not undergoing hemodialysis during a hospital admission. Although our findings support that IV iron treatment is safe among patients with concomitant infection and iron deficiency, this finding may not be the case for all clinical subgroups.
Conclusions: This study showed that when patients were administered IV iron in the setting of acute bacterial infection in our facility, most patients did not have negative outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


