Paul Casabianca, Marc Massetti, François-Emery Cotte, Romain Moreau, Sarah Kassahun, Prianka Singh, Inkyu Kim, Anne-Françoise Gaudin, Guillaume Piessen, Henri Leleu
{"title":"法国对已切除食管癌或胃食管交界癌患者进行 Nivolumab 辅助治疗的成本效益分析。","authors":"Paul Casabianca, Marc Massetti, François-Emery Cotte, Romain Moreau, Sarah Kassahun, Prianka Singh, Inkyu Kim, Anne-Françoise Gaudin, Guillaume Piessen, Henri Leleu","doi":"10.1007/s41669-024-00500-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Esophageal and gastroesophageal junction cancer (EC/GEJC) is a poor prognosis disease with a high risk of recurrence even in patients curatively resected. Adjuvant nivolumab is currently used for patients with completely resected (R0) EC/GEJC who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. This study aimed to determine the cost effectiveness of nivolumab in this indication in France according to the collective perspective excluding indirect costs.</p><p><strong>Materials and methods: </strong>A simplified four-health-state semi-Markov model was developed to model EC/GEJC patients who have residual disease after neoadjuvant chemoradiotherapy followed by R0 over a 15-year time horizon, comparing adjuvant nivolumab versus surveillance, which was the recommended French clinical practice before immunotherapy arrival. Time-to-recurrence (TTR) from CheckMate 577 was used to inform transition from disease-free to post-recurrence health state; patients who recurred were split according to the distribution of type of recurrence observed during the trial. Post-recurrence survival (PRS) according to the type of recurrence was derived from a real-world registry.</p><p><strong>Results: </strong>Adjuvant treatment with nivolumab led to an incremental survival gain of 1.19 years (+ 34%), mostly in the disease-free state, an incremental cost of €48,634 and QALY of 0.98 resulting in an incremental cost-utility ratio (ICUR) of €49,572/QALY with limited uncertainty. 'Cure assumption' at 5 years had an important impact on the results (€41,115/QALY; - 17%), as that tends to increase life-years and QALYs while costs remain the same. Probabilistic sensitivity analyses confirmed reference ICUR (€52,542/QALY) with 80% probability of nivolumab being cost effective at a willingness-to-pay threshold of €75,000/QALY.</p><p><strong>Conclusions: </strong>Our analysis suggests that adjuvant nivolumab is cost effective in the treatment of EC/GEJC patients who have residual disease after neoadjuvant CRT followed by R0 resection. Compared with previously evaluated cost-effectiveness analyses for other immune-checkpoint inhibitors indicated in metastatic settings, ICUR appears particularly low in this early setting thanks to the important impact on health outcomes and capped treatment duration.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"689-699"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362429/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Cost-Effectiveness Analysis of Adjuvant Nivolumab for Patients with Resected Esophageal Cancer or Gastroesophageal Junction Cancer in France.\",\"authors\":\"Paul Casabianca, Marc Massetti, François-Emery Cotte, Romain Moreau, Sarah Kassahun, Prianka Singh, Inkyu Kim, Anne-Françoise Gaudin, Guillaume Piessen, Henri Leleu\",\"doi\":\"10.1007/s41669-024-00500-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Esophageal and gastroesophageal junction cancer (EC/GEJC) is a poor prognosis disease with a high risk of recurrence even in patients curatively resected. Adjuvant nivolumab is currently used for patients with completely resected (R0) EC/GEJC who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. This study aimed to determine the cost effectiveness of nivolumab in this indication in France according to the collective perspective excluding indirect costs.</p><p><strong>Materials and methods: </strong>A simplified four-health-state semi-Markov model was developed to model EC/GEJC patients who have residual disease after neoadjuvant chemoradiotherapy followed by R0 over a 15-year time horizon, comparing adjuvant nivolumab versus surveillance, which was the recommended French clinical practice before immunotherapy arrival. Time-to-recurrence (TTR) from CheckMate 577 was used to inform transition from disease-free to post-recurrence health state; patients who recurred were split according to the distribution of type of recurrence observed during the trial. Post-recurrence survival (PRS) according to the type of recurrence was derived from a real-world registry.</p><p><strong>Results: </strong>Adjuvant treatment with nivolumab led to an incremental survival gain of 1.19 years (+ 34%), mostly in the disease-free state, an incremental cost of €48,634 and QALY of 0.98 resulting in an incremental cost-utility ratio (ICUR) of €49,572/QALY with limited uncertainty. 'Cure assumption' at 5 years had an important impact on the results (€41,115/QALY; - 17%), as that tends to increase life-years and QALYs while costs remain the same. Probabilistic sensitivity analyses confirmed reference ICUR (€52,542/QALY) with 80% probability of nivolumab being cost effective at a willingness-to-pay threshold of €75,000/QALY.</p><p><strong>Conclusions: </strong>Our analysis suggests that adjuvant nivolumab is cost effective in the treatment of EC/GEJC patients who have residual disease after neoadjuvant CRT followed by R0 resection. Compared with previously evaluated cost-effectiveness analyses for other immune-checkpoint inhibitors indicated in metastatic settings, ICUR appears particularly low in this early setting thanks to the important impact on health outcomes and capped treatment duration.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"689-699\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362429/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-024-00500-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00500-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
A Cost-Effectiveness Analysis of Adjuvant Nivolumab for Patients with Resected Esophageal Cancer or Gastroesophageal Junction Cancer in France.
Introduction: Esophageal and gastroesophageal junction cancer (EC/GEJC) is a poor prognosis disease with a high risk of recurrence even in patients curatively resected. Adjuvant nivolumab is currently used for patients with completely resected (R0) EC/GEJC who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. This study aimed to determine the cost effectiveness of nivolumab in this indication in France according to the collective perspective excluding indirect costs.
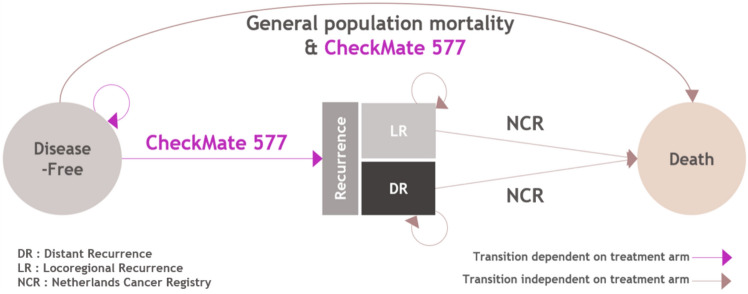
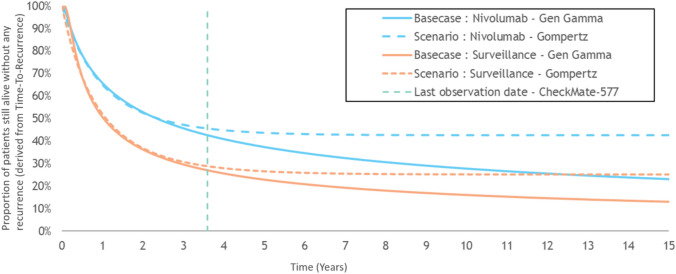
Materials and methods: A simplified four-health-state semi-Markov model was developed to model EC/GEJC patients who have residual disease after neoadjuvant chemoradiotherapy followed by R0 over a 15-year time horizon, comparing adjuvant nivolumab versus surveillance, which was the recommended French clinical practice before immunotherapy arrival. Time-to-recurrence (TTR) from CheckMate 577 was used to inform transition from disease-free to post-recurrence health state; patients who recurred were split according to the distribution of type of recurrence observed during the trial. Post-recurrence survival (PRS) according to the type of recurrence was derived from a real-world registry.
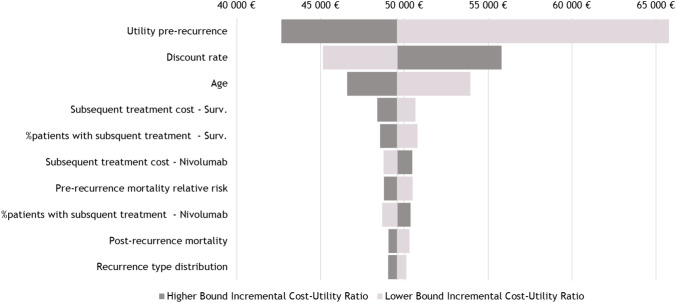
Results: Adjuvant treatment with nivolumab led to an incremental survival gain of 1.19 years (+ 34%), mostly in the disease-free state, an incremental cost of €48,634 and QALY of 0.98 resulting in an incremental cost-utility ratio (ICUR) of €49,572/QALY with limited uncertainty. 'Cure assumption' at 5 years had an important impact on the results (€41,115/QALY; - 17%), as that tends to increase life-years and QALYs while costs remain the same. Probabilistic sensitivity analyses confirmed reference ICUR (€52,542/QALY) with 80% probability of nivolumab being cost effective at a willingness-to-pay threshold of €75,000/QALY.
Conclusions: Our analysis suggests that adjuvant nivolumab is cost effective in the treatment of EC/GEJC patients who have residual disease after neoadjuvant CRT followed by R0 resection. Compared with previously evaluated cost-effectiveness analyses for other immune-checkpoint inhibitors indicated in metastatic settings, ICUR appears particularly low in this early setting thanks to the important impact on health outcomes and capped treatment duration.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


