Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman
{"title":"评估骨髓瘤患者的虚弱程度:追求简单可能会牺牲预测临床结果的准确性。","authors":"Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman","doi":"10.1002/hem3.85","DOIUrl":null,"url":null,"abstract":"<p>In 2015, the International Myeloma Working Group (IMWG) introduced a frailty index (IMWG-FI), as a means to quantify fragility of patients with multiple myeloma (MM). This index categorizes patients into three groups: fit, intermediate-fit, or frail, based on age, comorbidities, and the level of assistance for (instrumental) daily activities ((i)ADL). Scores on the IMWG-FI range from zero to five points. A score of zero designates patients as fit, a score of one indicates intermediate-fit, and a score between two and five denotes frail. Three-year overall survival rates were 84% in fit patients, 76% in intermediate-fit patients (hazard ratio [HR]: 1.61; 95% confidence interval (CI): 1.02–2.56; <i>p</i> = 0.042). and 57% in frail patients (HR: 3.57; 95% CI: 2.37–5.39; <i>p</i> < 0.001). In addition, frail patients had a significantly inferior progression-free survival (PFS), a higher tendency to discontinue treatment, and experienced more nonhematologic toxicity, compared to fit patients, which was found to be independent of ISS stage, chromosomal abnormalities, and type of therapy.<span><sup>1</sup></span></p><p>In response to the time-consuming nature and feasibility challenges of assessing the (i)ADL scales in clinical studies, the Simplified Frailty Index (Simplified-FI) emerged in 2020. It substitutes daily activities with the World Health Organization Performance Status (WHO-PS). Also the Simplified-FI underscored that frail patients faced an adverse outcome.<span><sup>2</sup></span> Post hoc frailty subgroup analyses in the MAIA and the ALCYONE trials, utilizing the Simplified-FI showed that frail patients had an inferior OS (41.2 months) compared to non-frail (fit and intermediate-fit combined; 70.1 months) patients, particularly evident in the daratumumab-arm of both studies (HR: 1.86; 95% CI: 1.63–2.12; <i>p</i> < 0.0001).<span><sup>3, 4</sup></span></p><p>While both the IMWG-FI and the Simplified-FI categorize patients as fit, intermediate-fit, or frail, the exact alignment of these groups remains uncertain. The question is whether physician-reported WHO-PS can actually replace patient-reported (i)ADL, which better reflects underlying physical, cognitive, or functional problems. There is reason to question concordance as variances in patient outcomes under the same treatment regimen have been noted, depending on which frailty index was employed. For example, intermediate-fit patients, as classified by the Simplified-FI, achieved a median PFS of over 36 months with continuous lenalidomide/dexamethasone in the MAIA study, while patients classified as intermediate-fit according to the IMWG-FI treated with the same regimen in an Italian study had a median PFS of only 18.3 months, suggesting that the Simplified-FI identifies a less vulnerable intermediate-fit patient population.<span><sup>3, 5</sup></span> Given expert recommendations advocating for treatment adjustments based on frailty, it is crucial to acknowledge potential disparities between these two scores.<span><sup>6</sup></span> Our analysis delves into the frequency of divergent patient classifications between the two frailty indices and their impact on clinical outcomes.</p><p>For this analysis, the data of the HOVON 123 and HOVON 143 studies were pooled. In the HOVON 123 study, 238 nontransplant eligible newly diagnosed multiple myeloma (NTE-NDMM) patients ≥75 years old were treated with nine cycles of dose-adjusted melphalan, prednisone, and bortezomib.<span><sup>7</sup></span> In the HOVON 143 study, 130 NTE-NDMM patients were treated with nine cycles of ixazomib, daratumumab, and low-dose-dexamethasone (Ixa-Dara-dex) followed by a maintenance phase of Ixa-Dara-dex until progression for a maximum of 2 years.<span><sup>8, 9</sup></span> Patients in whom frailty status was unknown were excluded from analysis. Patients were classified as fit, intermediate-fit, or frail, using both indices, and subsequently discordance rates were determined. Patient- and disease characteristics and clinical outcomes (PFS, PFS2, OS, and treatment discontinuation) were compared between patients with discordant or concordant frailty classification. Depending on the type of variable, the chi-squared test, Fisher's exact test, and Wilcoxon Ranked sum test were used for statistical testing of differences between the different patient groups. To rule out a trial effect on PFS, PFS2, or OS, we performed a multivariate cox regression analysis including trial effect.</p><p>In total, 368 patients were included in both studies. The IMWG-FI and/or Simplified-FI status were missing in 19 patients. As fit patients were underrepresented (<i>n</i> = 10), this subgroup was excluded. Therefore, 339 patients were included in the analysis.</p><p>According to the Simplified-FI, 67 patients (20%) were intermediate-fit and 272 patients (80%) were frail, which was 131 (39%) and 208 (61%) according to the IMWG-FI, respectively. The discordance rate between the two frailty indices was 22.4% (76/339). Of the 67 patients who were intermediate-fit according to the Simplified-FI, six (9%) patients would be classified (further mentioned “reclassified”) as frail when using the gold standard IMWG-FI, whereas 61 patients (91%) were classified intermediate-fit independent of the FI that was used. Of the 272 patients who were frail based on the Simplified-FI, 70 patients (26%) would be reclassified to intermediate-fit when using the IMWG-FI, whereas 202 patients (74%) were classified frail by both indices (Supporting Information S1: Figure 1).</p><p>The limited number of patients that shifted from intermediate-fit based on the Simplified-FI to frail patients according to the IMWG-FI (<i>n</i> = 6) hampered meaningful comparisons with patients with concordant scores. The 70 patients who were reclassified from frail according to the Simplified-FI to intermediate-fit according to the IMWG-FI were significantly younger, more frequently independent in ADL and IADL, exhibited fewer comorbidities, and had a better WHO-PS, a favorable ISS stage and lower β2-microglobuline, as compared to patients classified as frail regardless of the FI used. These 70 reclassified patients were comparable to those classified as intermediate-fit irrespective of the FI employed, except for an inferior WHO-PS, as was expected as they were defined frail based on an inferior WHO-PS in the Simplified-FI (Table 1). Furthermore, the PFS, PFS2, and OS of these reclassified 70 patients were comparable to patients who were intermediate-fit independent of the FI that was used; median PFS 16.5 months (95% CI: 13.8–21.6) versus 18.5 months (95% CI: 16.8–25.3) and median PFS2 40.0 months (95% CI: 34.3–64.8) versus 46.7 months (95% CI: 37.3–64.0). Moreover, 61% (95% CI: 50–74) were alive at 4 years versus 66% (95% CI: 55–80), respectively (Figure 1A, Supporting Information S1: Figure 2A and 3A). In contrast, the median PFS2 and OS of those 70 patients were different from patients deemed frail by both indices (<i>n</i> = 202); median PFS2 (29.1 months (95% CI: 23.8–35.0), HR 0.66 (95% CI: 0.47–0.91), <i>p</i> = 0.01), and median OS (34.1 months (95% CI: 29.5–40.2), HR 0.55 (95% CI: 0.39–0.80), <i>p</i> = 0.0012) (Figure 1B, Supporting Information S1: Table 1 and Figures 2B and 3B). Median PFS was comparable (16.4 months; 95% CI: 14.3–17.7). There was no significant trial effect on PFS, PFS2, or OS. These findings indicate that the IMWG-FI outperforms the Simplified-FI in predicting outcomes. However, this superiority was not evident in treatment discontinuation rate at 3, 6, and 9 cycles, as comparable numbers were observed between the 70 reclassified patients and those with a concordant classification (Supporting Information S1: Table 2).</p><p>To the best of our knowledge, this is the first study comparing two pivotal frailty assessment tools in MM; the gold standard IMWG-FI and the Simplified-FI in a large group of patients who were included in two prospective HOVON trials designed for NTE-NDMM patients. Our analysis reveals a significant discordance rate, with the Simplified-FI more frequently classifying patients as frail compared to the gold-standard IMWG-FI. An in-depth analysis of the 70 reclassified patients (frail by Simplified-FI, intermediate-fit by IMWG-FI) regarding patient- and disease characteristics, and clinical outcome, underscores that they closely resemble intermediate-fit patients. Therefore, this discrepancy prompts a crucial question regarding the Simplified-FI for clinical application.</p><p>The ultimate goal of frailty assessment is to identify patients who would or would not benefit from dose-adjusted treatment. In those who are expected not to benefit from standard treatment, the value of frailty-adjusted treatment approaches is currently being investigated. However, while awaiting the results of randomized clinical trials, such as the frailty-adjusted FiTNEss trial, frailty already guides treatment decision in clinical practice.<span><sup>6, 10</sup></span> The adoption of the Simplified-FI may pose a risk to patients by introducing intermediate-fit individuals, as identified by the IMWG-FI, into the vulnerable patient population. This could result in unjustified withholding of treatment for these patients.</p><p>Notably, the exclusion of fit patients from our analysis precludes conclusions about disparities between both FI's over the whole spectrum of frailty. Since our analysis shows that patients tend to report to be more (i)ADL-independent compared to the physician-reported WHO performance status, this may lead to the categorization of more intermediate-fit, or even frail patients based on the Simplified-FI, whereas the IMWG-FI would have classified them as fit. This would strengthen our plea for using the IMWG-FI and therefore this hypothesis warrants testing by applying the Simplified-FI on the original IMWG-FI cohort, in which over one-third of patients were deemed fit.<span><sup>1</sup></span></p><p>Both scores have in common that patients aged over 80 years, without comorbidities or impairments in (I)ADL and a WHO-PS of 0, are frail based on age only. Whether these patients have the same prognosis as patients aged over 80 with comorbidities, impairments in (I)ADL, or a WHO-PS of 1 or higher (ultra-frail), regarding survival and treatment tolerability is at least questionable. We showed that patients being frail based on age only tend to have a superior PFS as compared to ultra-frail patients, although not statistically significant which might be due to small numbers. In contrast, in the original IMWG-FI cohort, patients being frail based on age only had comparable outcome as patients being frail because of geriatric impairments with or without age over 80.<span><sup>8, 11</sup></span> Therefore future studies are warranted to define the impact of being ultra-frail on prognosis.</p><p>We here show that the Simplified-FI identifies more patients as frail, including patients that would have been intermediate-fit when the gold standard IMWG-FI was used. These reclassified patients closely resemble those consistently intermediate-fit patients based on both indices, not only in terms of patient- and disease characteristics but also in clinical outcomes. To mitigate the risk of undertreating incorrectly classified patients, our study strongly advocates for the use of the IMWG-FI over the Simplified-FI in clinical practice.</p><p>Kazimierz Groen, Febe Smits, Kazem Nasserinejad, and Sonja Zweegman designed the research. Kazem Nasserinejad accessed and verified the data. Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, and Sonja Zweegman analyzed the data. Kazimierz Groen, Febe Smits, and Sonja Zweegman wrote the paper. Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman provided study patients. All authors approved the final version of the manuscript and are accountable for all aspects of the work.</p><p>Kazimierz Groen: BMS and Beigene: speakers bureau (no personal funding). Febe Smits: No conflicts of interest. Kazem Nasserinejad: No conflicts of interest. Mark-David Levin: Support for attending meetings and/or travel: Janssen, Takeda. Josien C. Regelink: No conflicts of interest. Gert-Jan Timmers: Participation on an Advisory Board: Novartis; Travel, Accommodations, Expenses; Novartis, Janssen. Esther G. M. de Waal: No conflicts of interest. Matthijs Westerman: No conflicts of interest. Gerjo A. Velders: No conflicts of interest. Koen de Heer: No conflicts of interest. Rineke B. L. Leys: No conflicts of interest. Roel J. W. van Kampen: No conflicts of interest. Claudia A. M. Stege: Speaker's Bureau: Sanofi, Celgene/Bristol Myers Squibb, Takeda; Consulting or Advisory Role: Sanofi, Janssen. Maarten R. Seefat: No conflicts of interest. Inger S. Nijhof: Payment or honoraria for lectures, presentations, or educational events: Janssen, Celgene/Bristol Myers Squibb, Sanofi. Ellen van der Spek: Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Janssen. Saskia K. Klein: No conflicts of interest. Niels W. C. J. van de Donk: Consulting or Advisory Role: Janssen, Celgene, Bristol Myers Squibb, Novartis, Amgen, Servier, Takeda, Bayer, Roche, Pfizer, Abbvie, Adaptive (no personal funding); Research Funding: Janssen, Celgene, Amgen, Novartis, Bristol Myers Squibb, Cellectis. Paula F. Ypma: Payment or honoraria for presentations: Janssen; Support for attending meetings and/or travel: Janssen. Sonja Zweegman: Consulting or Advisory Role: Janssen-Cilag, Takeda, Celgene/Bristol Myers Squibb, Sanofi, Oncopeptides (no personal funding); Research Funding: Janssen, Takeda.</p><p>Dutch Cancer Society (KWF), Janssen and Takeda.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11223651/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing frailty in myeloma: The pursuit of simplicity may sacrifice precision of predicting clinical outcomes\",\"authors\":\"Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman\",\"doi\":\"10.1002/hem3.85\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In 2015, the International Myeloma Working Group (IMWG) introduced a frailty index (IMWG-FI), as a means to quantify fragility of patients with multiple myeloma (MM). This index categorizes patients into three groups: fit, intermediate-fit, or frail, based on age, comorbidities, and the level of assistance for (instrumental) daily activities ((i)ADL). Scores on the IMWG-FI range from zero to five points. A score of zero designates patients as fit, a score of one indicates intermediate-fit, and a score between two and five denotes frail. Three-year overall survival rates were 84% in fit patients, 76% in intermediate-fit patients (hazard ratio [HR]: 1.61; 95% confidence interval (CI): 1.02–2.56; <i>p</i> = 0.042). and 57% in frail patients (HR: 3.57; 95% CI: 2.37–5.39; <i>p</i> < 0.001). In addition, frail patients had a significantly inferior progression-free survival (PFS), a higher tendency to discontinue treatment, and experienced more nonhematologic toxicity, compared to fit patients, which was found to be independent of ISS stage, chromosomal abnormalities, and type of therapy.<span><sup>1</sup></span></p><p>In response to the time-consuming nature and feasibility challenges of assessing the (i)ADL scales in clinical studies, the Simplified Frailty Index (Simplified-FI) emerged in 2020. It substitutes daily activities with the World Health Organization Performance Status (WHO-PS). Also the Simplified-FI underscored that frail patients faced an adverse outcome.<span><sup>2</sup></span> Post hoc frailty subgroup analyses in the MAIA and the ALCYONE trials, utilizing the Simplified-FI showed that frail patients had an inferior OS (41.2 months) compared to non-frail (fit and intermediate-fit combined; 70.1 months) patients, particularly evident in the daratumumab-arm of both studies (HR: 1.86; 95% CI: 1.63–2.12; <i>p</i> < 0.0001).<span><sup>3, 4</sup></span></p><p>While both the IMWG-FI and the Simplified-FI categorize patients as fit, intermediate-fit, or frail, the exact alignment of these groups remains uncertain. The question is whether physician-reported WHO-PS can actually replace patient-reported (i)ADL, which better reflects underlying physical, cognitive, or functional problems. There is reason to question concordance as variances in patient outcomes under the same treatment regimen have been noted, depending on which frailty index was employed. For example, intermediate-fit patients, as classified by the Simplified-FI, achieved a median PFS of over 36 months with continuous lenalidomide/dexamethasone in the MAIA study, while patients classified as intermediate-fit according to the IMWG-FI treated with the same regimen in an Italian study had a median PFS of only 18.3 months, suggesting that the Simplified-FI identifies a less vulnerable intermediate-fit patient population.<span><sup>3, 5</sup></span> Given expert recommendations advocating for treatment adjustments based on frailty, it is crucial to acknowledge potential disparities between these two scores.<span><sup>6</sup></span> Our analysis delves into the frequency of divergent patient classifications between the two frailty indices and their impact on clinical outcomes.</p><p>For this analysis, the data of the HOVON 123 and HOVON 143 studies were pooled. In the HOVON 123 study, 238 nontransplant eligible newly diagnosed multiple myeloma (NTE-NDMM) patients ≥75 years old were treated with nine cycles of dose-adjusted melphalan, prednisone, and bortezomib.<span><sup>7</sup></span> In the HOVON 143 study, 130 NTE-NDMM patients were treated with nine cycles of ixazomib, daratumumab, and low-dose-dexamethasone (Ixa-Dara-dex) followed by a maintenance phase of Ixa-Dara-dex until progression for a maximum of 2 years.<span><sup>8, 9</sup></span> Patients in whom frailty status was unknown were excluded from analysis. Patients were classified as fit, intermediate-fit, or frail, using both indices, and subsequently discordance rates were determined. Patient- and disease characteristics and clinical outcomes (PFS, PFS2, OS, and treatment discontinuation) were compared between patients with discordant or concordant frailty classification. Depending on the type of variable, the chi-squared test, Fisher's exact test, and Wilcoxon Ranked sum test were used for statistical testing of differences between the different patient groups. To rule out a trial effect on PFS, PFS2, or OS, we performed a multivariate cox regression analysis including trial effect.</p><p>In total, 368 patients were included in both studies. The IMWG-FI and/or Simplified-FI status were missing in 19 patients. As fit patients were underrepresented (<i>n</i> = 10), this subgroup was excluded. Therefore, 339 patients were included in the analysis.</p><p>According to the Simplified-FI, 67 patients (20%) were intermediate-fit and 272 patients (80%) were frail, which was 131 (39%) and 208 (61%) according to the IMWG-FI, respectively. The discordance rate between the two frailty indices was 22.4% (76/339). Of the 67 patients who were intermediate-fit according to the Simplified-FI, six (9%) patients would be classified (further mentioned “reclassified”) as frail when using the gold standard IMWG-FI, whereas 61 patients (91%) were classified intermediate-fit independent of the FI that was used. Of the 272 patients who were frail based on the Simplified-FI, 70 patients (26%) would be reclassified to intermediate-fit when using the IMWG-FI, whereas 202 patients (74%) were classified frail by both indices (Supporting Information S1: Figure 1).</p><p>The limited number of patients that shifted from intermediate-fit based on the Simplified-FI to frail patients according to the IMWG-FI (<i>n</i> = 6) hampered meaningful comparisons with patients with concordant scores. The 70 patients who were reclassified from frail according to the Simplified-FI to intermediate-fit according to the IMWG-FI were significantly younger, more frequently independent in ADL and IADL, exhibited fewer comorbidities, and had a better WHO-PS, a favorable ISS stage and lower β2-microglobuline, as compared to patients classified as frail regardless of the FI used. These 70 reclassified patients were comparable to those classified as intermediate-fit irrespective of the FI employed, except for an inferior WHO-PS, as was expected as they were defined frail based on an inferior WHO-PS in the Simplified-FI (Table 1). Furthermore, the PFS, PFS2, and OS of these reclassified 70 patients were comparable to patients who were intermediate-fit independent of the FI that was used; median PFS 16.5 months (95% CI: 13.8–21.6) versus 18.5 months (95% CI: 16.8–25.3) and median PFS2 40.0 months (95% CI: 34.3–64.8) versus 46.7 months (95% CI: 37.3–64.0). Moreover, 61% (95% CI: 50–74) were alive at 4 years versus 66% (95% CI: 55–80), respectively (Figure 1A, Supporting Information S1: Figure 2A and 3A). In contrast, the median PFS2 and OS of those 70 patients were different from patients deemed frail by both indices (<i>n</i> = 202); median PFS2 (29.1 months (95% CI: 23.8–35.0), HR 0.66 (95% CI: 0.47–0.91), <i>p</i> = 0.01), and median OS (34.1 months (95% CI: 29.5–40.2), HR 0.55 (95% CI: 0.39–0.80), <i>p</i> = 0.0012) (Figure 1B, Supporting Information S1: Table 1 and Figures 2B and 3B). Median PFS was comparable (16.4 months; 95% CI: 14.3–17.7). There was no significant trial effect on PFS, PFS2, or OS. These findings indicate that the IMWG-FI outperforms the Simplified-FI in predicting outcomes. However, this superiority was not evident in treatment discontinuation rate at 3, 6, and 9 cycles, as comparable numbers were observed between the 70 reclassified patients and those with a concordant classification (Supporting Information S1: Table 2).</p><p>To the best of our knowledge, this is the first study comparing two pivotal frailty assessment tools in MM; the gold standard IMWG-FI and the Simplified-FI in a large group of patients who were included in two prospective HOVON trials designed for NTE-NDMM patients. Our analysis reveals a significant discordance rate, with the Simplified-FI more frequently classifying patients as frail compared to the gold-standard IMWG-FI. An in-depth analysis of the 70 reclassified patients (frail by Simplified-FI, intermediate-fit by IMWG-FI) regarding patient- and disease characteristics, and clinical outcome, underscores that they closely resemble intermediate-fit patients. Therefore, this discrepancy prompts a crucial question regarding the Simplified-FI for clinical application.</p><p>The ultimate goal of frailty assessment is to identify patients who would or would not benefit from dose-adjusted treatment. In those who are expected not to benefit from standard treatment, the value of frailty-adjusted treatment approaches is currently being investigated. However, while awaiting the results of randomized clinical trials, such as the frailty-adjusted FiTNEss trial, frailty already guides treatment decision in clinical practice.<span><sup>6, 10</sup></span> The adoption of the Simplified-FI may pose a risk to patients by introducing intermediate-fit individuals, as identified by the IMWG-FI, into the vulnerable patient population. This could result in unjustified withholding of treatment for these patients.</p><p>Notably, the exclusion of fit patients from our analysis precludes conclusions about disparities between both FI's over the whole spectrum of frailty. Since our analysis shows that patients tend to report to be more (i)ADL-independent compared to the physician-reported WHO performance status, this may lead to the categorization of more intermediate-fit, or even frail patients based on the Simplified-FI, whereas the IMWG-FI would have classified them as fit. This would strengthen our plea for using the IMWG-FI and therefore this hypothesis warrants testing by applying the Simplified-FI on the original IMWG-FI cohort, in which over one-third of patients were deemed fit.<span><sup>1</sup></span></p><p>Both scores have in common that patients aged over 80 years, without comorbidities or impairments in (I)ADL and a WHO-PS of 0, are frail based on age only. Whether these patients have the same prognosis as patients aged over 80 with comorbidities, impairments in (I)ADL, or a WHO-PS of 1 or higher (ultra-frail), regarding survival and treatment tolerability is at least questionable. We showed that patients being frail based on age only tend to have a superior PFS as compared to ultra-frail patients, although not statistically significant which might be due to small numbers. In contrast, in the original IMWG-FI cohort, patients being frail based on age only had comparable outcome as patients being frail because of geriatric impairments with or without age over 80.<span><sup>8, 11</sup></span> Therefore future studies are warranted to define the impact of being ultra-frail on prognosis.</p><p>We here show that the Simplified-FI identifies more patients as frail, including patients that would have been intermediate-fit when the gold standard IMWG-FI was used. These reclassified patients closely resemble those consistently intermediate-fit patients based on both indices, not only in terms of patient- and disease characteristics but also in clinical outcomes. To mitigate the risk of undertreating incorrectly classified patients, our study strongly advocates for the use of the IMWG-FI over the Simplified-FI in clinical practice.</p><p>Kazimierz Groen, Febe Smits, Kazem Nasserinejad, and Sonja Zweegman designed the research. Kazem Nasserinejad accessed and verified the data. Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, and Sonja Zweegman analyzed the data. Kazimierz Groen, Febe Smits, and Sonja Zweegman wrote the paper. Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman provided study patients. All authors approved the final version of the manuscript and are accountable for all aspects of the work.</p><p>Kazimierz Groen: BMS and Beigene: speakers bureau (no personal funding). Febe Smits: No conflicts of interest. Kazem Nasserinejad: No conflicts of interest. Mark-David Levin: Support for attending meetings and/or travel: Janssen, Takeda. Josien C. Regelink: No conflicts of interest. Gert-Jan Timmers: Participation on an Advisory Board: Novartis; Travel, Accommodations, Expenses; Novartis, Janssen. Esther G. M. de Waal: No conflicts of interest. Matthijs Westerman: No conflicts of interest. Gerjo A. Velders: No conflicts of interest. Koen de Heer: No conflicts of interest. Rineke B. L. Leys: No conflicts of interest. Roel J. W. van Kampen: No conflicts of interest. Claudia A. M. Stege: Speaker's Bureau: Sanofi, Celgene/Bristol Myers Squibb, Takeda; Consulting or Advisory Role: Sanofi, Janssen. Maarten R. Seefat: No conflicts of interest. Inger S. Nijhof: Payment or honoraria for lectures, presentations, or educational events: Janssen, Celgene/Bristol Myers Squibb, Sanofi. Ellen van der Spek: Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Janssen. Saskia K. Klein: No conflicts of interest. Niels W. C. J. van de Donk: Consulting or Advisory Role: Janssen, Celgene, Bristol Myers Squibb, Novartis, Amgen, Servier, Takeda, Bayer, Roche, Pfizer, Abbvie, Adaptive (no personal funding); Research Funding: Janssen, Celgene, Amgen, Novartis, Bristol Myers Squibb, Cellectis. Paula F. Ypma: Payment or honoraria for presentations: Janssen; Support for attending meetings and/or travel: Janssen. Sonja Zweegman: Consulting or Advisory Role: Janssen-Cilag, Takeda, Celgene/Bristol Myers Squibb, Sanofi, Oncopeptides (no personal funding); Research Funding: Janssen, Takeda.</p><p>Dutch Cancer Society (KWF), Janssen and Takeda.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 7\",\"pages\":\"\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2024-07-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11223651/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.85\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.85","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Assessing frailty in myeloma: The pursuit of simplicity may sacrifice precision of predicting clinical outcomes
In 2015, the International Myeloma Working Group (IMWG) introduced a frailty index (IMWG-FI), as a means to quantify fragility of patients with multiple myeloma (MM). This index categorizes patients into three groups: fit, intermediate-fit, or frail, based on age, comorbidities, and the level of assistance for (instrumental) daily activities ((i)ADL). Scores on the IMWG-FI range from zero to five points. A score of zero designates patients as fit, a score of one indicates intermediate-fit, and a score between two and five denotes frail. Three-year overall survival rates were 84% in fit patients, 76% in intermediate-fit patients (hazard ratio [HR]: 1.61; 95% confidence interval (CI): 1.02–2.56; p = 0.042). and 57% in frail patients (HR: 3.57; 95% CI: 2.37–5.39; p < 0.001). In addition, frail patients had a significantly inferior progression-free survival (PFS), a higher tendency to discontinue treatment, and experienced more nonhematologic toxicity, compared to fit patients, which was found to be independent of ISS stage, chromosomal abnormalities, and type of therapy.1
In response to the time-consuming nature and feasibility challenges of assessing the (i)ADL scales in clinical studies, the Simplified Frailty Index (Simplified-FI) emerged in 2020. It substitutes daily activities with the World Health Organization Performance Status (WHO-PS). Also the Simplified-FI underscored that frail patients faced an adverse outcome.2 Post hoc frailty subgroup analyses in the MAIA and the ALCYONE trials, utilizing the Simplified-FI showed that frail patients had an inferior OS (41.2 months) compared to non-frail (fit and intermediate-fit combined; 70.1 months) patients, particularly evident in the daratumumab-arm of both studies (HR: 1.86; 95% CI: 1.63–2.12; p < 0.0001).3, 4
While both the IMWG-FI and the Simplified-FI categorize patients as fit, intermediate-fit, or frail, the exact alignment of these groups remains uncertain. The question is whether physician-reported WHO-PS can actually replace patient-reported (i)ADL, which better reflects underlying physical, cognitive, or functional problems. There is reason to question concordance as variances in patient outcomes under the same treatment regimen have been noted, depending on which frailty index was employed. For example, intermediate-fit patients, as classified by the Simplified-FI, achieved a median PFS of over 36 months with continuous lenalidomide/dexamethasone in the MAIA study, while patients classified as intermediate-fit according to the IMWG-FI treated with the same regimen in an Italian study had a median PFS of only 18.3 months, suggesting that the Simplified-FI identifies a less vulnerable intermediate-fit patient population.3, 5 Given expert recommendations advocating for treatment adjustments based on frailty, it is crucial to acknowledge potential disparities between these two scores.6 Our analysis delves into the frequency of divergent patient classifications between the two frailty indices and their impact on clinical outcomes.
For this analysis, the data of the HOVON 123 and HOVON 143 studies were pooled. In the HOVON 123 study, 238 nontransplant eligible newly diagnosed multiple myeloma (NTE-NDMM) patients ≥75 years old were treated with nine cycles of dose-adjusted melphalan, prednisone, and bortezomib.7 In the HOVON 143 study, 130 NTE-NDMM patients were treated with nine cycles of ixazomib, daratumumab, and low-dose-dexamethasone (Ixa-Dara-dex) followed by a maintenance phase of Ixa-Dara-dex until progression for a maximum of 2 years.8, 9 Patients in whom frailty status was unknown were excluded from analysis. Patients were classified as fit, intermediate-fit, or frail, using both indices, and subsequently discordance rates were determined. Patient- and disease characteristics and clinical outcomes (PFS, PFS2, OS, and treatment discontinuation) were compared between patients with discordant or concordant frailty classification. Depending on the type of variable, the chi-squared test, Fisher's exact test, and Wilcoxon Ranked sum test were used for statistical testing of differences between the different patient groups. To rule out a trial effect on PFS, PFS2, or OS, we performed a multivariate cox regression analysis including trial effect.
In total, 368 patients were included in both studies. The IMWG-FI and/or Simplified-FI status were missing in 19 patients. As fit patients were underrepresented (n = 10), this subgroup was excluded. Therefore, 339 patients were included in the analysis.
According to the Simplified-FI, 67 patients (20%) were intermediate-fit and 272 patients (80%) were frail, which was 131 (39%) and 208 (61%) according to the IMWG-FI, respectively. The discordance rate between the two frailty indices was 22.4% (76/339). Of the 67 patients who were intermediate-fit according to the Simplified-FI, six (9%) patients would be classified (further mentioned “reclassified”) as frail when using the gold standard IMWG-FI, whereas 61 patients (91%) were classified intermediate-fit independent of the FI that was used. Of the 272 patients who were frail based on the Simplified-FI, 70 patients (26%) would be reclassified to intermediate-fit when using the IMWG-FI, whereas 202 patients (74%) were classified frail by both indices (Supporting Information S1: Figure 1).
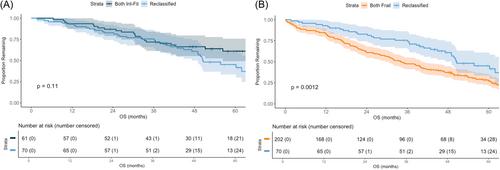
The limited number of patients that shifted from intermediate-fit based on the Simplified-FI to frail patients according to the IMWG-FI (n = 6) hampered meaningful comparisons with patients with concordant scores. The 70 patients who were reclassified from frail according to the Simplified-FI to intermediate-fit according to the IMWG-FI were significantly younger, more frequently independent in ADL and IADL, exhibited fewer comorbidities, and had a better WHO-PS, a favorable ISS stage and lower β2-microglobuline, as compared to patients classified as frail regardless of the FI used. These 70 reclassified patients were comparable to those classified as intermediate-fit irrespective of the FI employed, except for an inferior WHO-PS, as was expected as they were defined frail based on an inferior WHO-PS in the Simplified-FI (Table 1). Furthermore, the PFS, PFS2, and OS of these reclassified 70 patients were comparable to patients who were intermediate-fit independent of the FI that was used; median PFS 16.5 months (95% CI: 13.8–21.6) versus 18.5 months (95% CI: 16.8–25.3) and median PFS2 40.0 months (95% CI: 34.3–64.8) versus 46.7 months (95% CI: 37.3–64.0). Moreover, 61% (95% CI: 50–74) were alive at 4 years versus 66% (95% CI: 55–80), respectively (Figure 1A, Supporting Information S1: Figure 2A and 3A). In contrast, the median PFS2 and OS of those 70 patients were different from patients deemed frail by both indices (n = 202); median PFS2 (29.1 months (95% CI: 23.8–35.0), HR 0.66 (95% CI: 0.47–0.91), p = 0.01), and median OS (34.1 months (95% CI: 29.5–40.2), HR 0.55 (95% CI: 0.39–0.80), p = 0.0012) (Figure 1B, Supporting Information S1: Table 1 and Figures 2B and 3B). Median PFS was comparable (16.4 months; 95% CI: 14.3–17.7). There was no significant trial effect on PFS, PFS2, or OS. These findings indicate that the IMWG-FI outperforms the Simplified-FI in predicting outcomes. However, this superiority was not evident in treatment discontinuation rate at 3, 6, and 9 cycles, as comparable numbers were observed between the 70 reclassified patients and those with a concordant classification (Supporting Information S1: Table 2).
To the best of our knowledge, this is the first study comparing two pivotal frailty assessment tools in MM; the gold standard IMWG-FI and the Simplified-FI in a large group of patients who were included in two prospective HOVON trials designed for NTE-NDMM patients. Our analysis reveals a significant discordance rate, with the Simplified-FI more frequently classifying patients as frail compared to the gold-standard IMWG-FI. An in-depth analysis of the 70 reclassified patients (frail by Simplified-FI, intermediate-fit by IMWG-FI) regarding patient- and disease characteristics, and clinical outcome, underscores that they closely resemble intermediate-fit patients. Therefore, this discrepancy prompts a crucial question regarding the Simplified-FI for clinical application.
The ultimate goal of frailty assessment is to identify patients who would or would not benefit from dose-adjusted treatment. In those who are expected not to benefit from standard treatment, the value of frailty-adjusted treatment approaches is currently being investigated. However, while awaiting the results of randomized clinical trials, such as the frailty-adjusted FiTNEss trial, frailty already guides treatment decision in clinical practice.6, 10 The adoption of the Simplified-FI may pose a risk to patients by introducing intermediate-fit individuals, as identified by the IMWG-FI, into the vulnerable patient population. This could result in unjustified withholding of treatment for these patients.
Notably, the exclusion of fit patients from our analysis precludes conclusions about disparities between both FI's over the whole spectrum of frailty. Since our analysis shows that patients tend to report to be more (i)ADL-independent compared to the physician-reported WHO performance status, this may lead to the categorization of more intermediate-fit, or even frail patients based on the Simplified-FI, whereas the IMWG-FI would have classified them as fit. This would strengthen our plea for using the IMWG-FI and therefore this hypothesis warrants testing by applying the Simplified-FI on the original IMWG-FI cohort, in which over one-third of patients were deemed fit.1
Both scores have in common that patients aged over 80 years, without comorbidities or impairments in (I)ADL and a WHO-PS of 0, are frail based on age only. Whether these patients have the same prognosis as patients aged over 80 with comorbidities, impairments in (I)ADL, or a WHO-PS of 1 or higher (ultra-frail), regarding survival and treatment tolerability is at least questionable. We showed that patients being frail based on age only tend to have a superior PFS as compared to ultra-frail patients, although not statistically significant which might be due to small numbers. In contrast, in the original IMWG-FI cohort, patients being frail based on age only had comparable outcome as patients being frail because of geriatric impairments with or without age over 80.8, 11 Therefore future studies are warranted to define the impact of being ultra-frail on prognosis.
We here show that the Simplified-FI identifies more patients as frail, including patients that would have been intermediate-fit when the gold standard IMWG-FI was used. These reclassified patients closely resemble those consistently intermediate-fit patients based on both indices, not only in terms of patient- and disease characteristics but also in clinical outcomes. To mitigate the risk of undertreating incorrectly classified patients, our study strongly advocates for the use of the IMWG-FI over the Simplified-FI in clinical practice.
Kazimierz Groen, Febe Smits, Kazem Nasserinejad, and Sonja Zweegman designed the research. Kazem Nasserinejad accessed and verified the data. Kazimierz Groen, Febe Smits, Kazem Nasserinejad, Claudia A. M. Stege, Maarten R. Seefat, Inger S. Nijhof, and Sonja Zweegman analyzed the data. Kazimierz Groen, Febe Smits, and Sonja Zweegman wrote the paper. Mark-David Levin, Josien C. Regelink, Gert-Jan Timmers, Esther G. M. de Waal, Matthijs Westerman, Gerjo A. Velders, Koen de Heer, Rineke B. L. Leys, Roel J. W. van Kampen, Claudia A. M. Stege, Ellen van der Spek, Saskia K. Klein, Niels W. C. J. van de Donk, Paula F. Ypma, Sonja Zweegman provided study patients. All authors approved the final version of the manuscript and are accountable for all aspects of the work.
Kazimierz Groen: BMS and Beigene: speakers bureau (no personal funding). Febe Smits: No conflicts of interest. Kazem Nasserinejad: No conflicts of interest. Mark-David Levin: Support for attending meetings and/or travel: Janssen, Takeda. Josien C. Regelink: No conflicts of interest. Gert-Jan Timmers: Participation on an Advisory Board: Novartis; Travel, Accommodations, Expenses; Novartis, Janssen. Esther G. M. de Waal: No conflicts of interest. Matthijs Westerman: No conflicts of interest. Gerjo A. Velders: No conflicts of interest. Koen de Heer: No conflicts of interest. Rineke B. L. Leys: No conflicts of interest. Roel J. W. van Kampen: No conflicts of interest. Claudia A. M. Stege: Speaker's Bureau: Sanofi, Celgene/Bristol Myers Squibb, Takeda; Consulting or Advisory Role: Sanofi, Janssen. Maarten R. Seefat: No conflicts of interest. Inger S. Nijhof: Payment or honoraria for lectures, presentations, or educational events: Janssen, Celgene/Bristol Myers Squibb, Sanofi. Ellen van der Spek: Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Janssen. Saskia K. Klein: No conflicts of interest. Niels W. C. J. van de Donk: Consulting or Advisory Role: Janssen, Celgene, Bristol Myers Squibb, Novartis, Amgen, Servier, Takeda, Bayer, Roche, Pfizer, Abbvie, Adaptive (no personal funding); Research Funding: Janssen, Celgene, Amgen, Novartis, Bristol Myers Squibb, Cellectis. Paula F. Ypma: Payment or honoraria for presentations: Janssen; Support for attending meetings and/or travel: Janssen. Sonja Zweegman: Consulting or Advisory Role: Janssen-Cilag, Takeda, Celgene/Bristol Myers Squibb, Sanofi, Oncopeptides (no personal funding); Research Funding: Janssen, Takeda.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


