Aileen Zeng, Queenie Tang, Edel O'Hagan, Kirsten McCaffery, Kiran Ijaz, Juan C Quiroz, Ahmet Baki Kocaballi, Dana Rezazadegan, Ritu Trivedi, Joyce Siette, Timothy Shaw, Meredith Makeham, Aravinda Thiagalingam, Clara K Chow, Liliana Laranjo
{"title":"心房颤动治疗中数字患者决策支持工具的使用:系统回顾和荟萃分析。","authors":"Aileen Zeng, Queenie Tang, Edel O'Hagan, Kirsten McCaffery, Kiran Ijaz, Juan C Quiroz, Ahmet Baki Kocaballi, Dana Rezazadegan, Ritu Trivedi, Joyce Siette, Timothy Shaw, Meredith Makeham, Aravinda Thiagalingam, Clara K Chow, Liliana Laranjo","doi":"10.1136/bmjebm-2023-112820","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the effects of digital patient decision-support tools for atrial fibrillation (AF) treatment decisions in adults with AF.</p><p><strong>Study design: </strong>Systematic review and meta-analysis.</p><p><strong>Eligibility criteria: </strong>Eligible randomised controlled trials (RCTs) evaluated digital patient decision-support tools for AF treatment decisions in adults with AF.</p><p><strong>Information sources: </strong>We searched MEDLINE, EMBASE and Scopus from 2005 to 2023.Risk-of-bias (RoB) assessment: We assessed RoB using the Cochrane Risk of Bias Tool 2 for RCTs and cluster RCT and the ROBINS-I tool for quasi-experimental studies.</p><p><strong>Synthesis of results: </strong>We used random effects meta-analysis to synthesise decisional conflict and patient knowledge outcomes reported in RCTs. We performed narrative synthesis for all outcomes. The main outcomes of interest were decisional conflict and patient knowledge.</p><p><strong>Results: </strong>13 articles, reporting on 11 studies (4 RCTs, 1 cluster RCT and 6 quasi-experimental) met the inclusion criteria. There were 2714 participants across all studies (2372 in RCTs), of which 26% were women and the mean age was 71 years. Socioeconomically disadvantaged groups were poorly represented in the included studies. Seven studies (n=2508) focused on non-valvular AF and the mean CHAD2DS2-VASc across studies was 3.2 and for HAS-BLED 1.9. All tools focused on decisions regarding thromboembolic stroke prevention and most enabled calculation of individualised stroke risk. Tools were heterogeneous in features and functions; four tools were patient decision aids. The readability of content was reported in one study. Meta-analyses showed a reduction in decisional conflict (4 RCTs (n=2167); standardised mean difference -0.19; 95% CI -0.30 to -0.08; p=0.001; I<sup>2</sup>=26.5%; moderate certainty evidence) corresponding to a decrease in 12.4 units on a scale of 0 to 100 (95% CI -19.5 to -5.2) and improvement in patient knowledge (2 RCTs (n=1057); risk difference 0.72, 95% CI 0.68, 0.76, p<0.001; I<sup>2</sup>=0%; low certainty evidence) favouring digital patient decision-support tools compared with usual care. Four of the 11 tools were publicly available and 3 had been implemented in healthcare delivery.</p><p><strong>Conclusions: </strong>In the context of stroke prevention in AF, digital patient decision-support tools likely reduce decisional conflict and may result in little to no change in patient knowledge, compared with usual care. Future studies should leverage digital capabilities for increased personalisation and interactivity of the tools, with better consideration of health literacy and equity aspects. Additional robust trials and implementation studies are warranted.</p><p><strong>Prospero registration number: </strong>CRD42020218025.</p>","PeriodicalId":9059,"journal":{"name":"BMJ Evidence-Based Medicine","volume":" ","pages":"10-21"},"PeriodicalIF":7.6000,"publicationDate":"2025-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11874357/pdf/","citationCount":"0","resultStr":"{\"title\":\"Use of digital patient decision-support tools for atrial fibrillation treatments: a systematic review and meta-analysis.\",\"authors\":\"Aileen Zeng, Queenie Tang, Edel O'Hagan, Kirsten McCaffery, Kiran Ijaz, Juan C Quiroz, Ahmet Baki Kocaballi, Dana Rezazadegan, Ritu Trivedi, Joyce Siette, Timothy Shaw, Meredith Makeham, Aravinda Thiagalingam, Clara K Chow, Liliana Laranjo\",\"doi\":\"10.1136/bmjebm-2023-112820\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess the effects of digital patient decision-support tools for atrial fibrillation (AF) treatment decisions in adults with AF.</p><p><strong>Study design: </strong>Systematic review and meta-analysis.</p><p><strong>Eligibility criteria: </strong>Eligible randomised controlled trials (RCTs) evaluated digital patient decision-support tools for AF treatment decisions in adults with AF.</p><p><strong>Information sources: </strong>We searched MEDLINE, EMBASE and Scopus from 2005 to 2023.Risk-of-bias (RoB) assessment: We assessed RoB using the Cochrane Risk of Bias Tool 2 for RCTs and cluster RCT and the ROBINS-I tool for quasi-experimental studies.</p><p><strong>Synthesis of results: </strong>We used random effects meta-analysis to synthesise decisional conflict and patient knowledge outcomes reported in RCTs. We performed narrative synthesis for all outcomes. The main outcomes of interest were decisional conflict and patient knowledge.</p><p><strong>Results: </strong>13 articles, reporting on 11 studies (4 RCTs, 1 cluster RCT and 6 quasi-experimental) met the inclusion criteria. There were 2714 participants across all studies (2372 in RCTs), of which 26% were women and the mean age was 71 years. Socioeconomically disadvantaged groups were poorly represented in the included studies. Seven studies (n=2508) focused on non-valvular AF and the mean CHAD2DS2-VASc across studies was 3.2 and for HAS-BLED 1.9. All tools focused on decisions regarding thromboembolic stroke prevention and most enabled calculation of individualised stroke risk. Tools were heterogeneous in features and functions; four tools were patient decision aids. The readability of content was reported in one study. Meta-analyses showed a reduction in decisional conflict (4 RCTs (n=2167); standardised mean difference -0.19; 95% CI -0.30 to -0.08; p=0.001; I<sup>2</sup>=26.5%; moderate certainty evidence) corresponding to a decrease in 12.4 units on a scale of 0 to 100 (95% CI -19.5 to -5.2) and improvement in patient knowledge (2 RCTs (n=1057); risk difference 0.72, 95% CI 0.68, 0.76, p<0.001; I<sup>2</sup>=0%; low certainty evidence) favouring digital patient decision-support tools compared with usual care. Four of the 11 tools were publicly available and 3 had been implemented in healthcare delivery.</p><p><strong>Conclusions: </strong>In the context of stroke prevention in AF, digital patient decision-support tools likely reduce decisional conflict and may result in little to no change in patient knowledge, compared with usual care. Future studies should leverage digital capabilities for increased personalisation and interactivity of the tools, with better consideration of health literacy and equity aspects. Additional robust trials and implementation studies are warranted.</p><p><strong>Prospero registration number: </strong>CRD42020218025.</p>\",\"PeriodicalId\":9059,\"journal\":{\"name\":\"BMJ Evidence-Based Medicine\",\"volume\":\" \",\"pages\":\"10-21\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2025-01-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11874357/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Evidence-Based Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjebm-2023-112820\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Evidence-Based Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjebm-2023-112820","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Use of digital patient decision-support tools for atrial fibrillation treatments: a systematic review and meta-analysis.
Objectives: To assess the effects of digital patient decision-support tools for atrial fibrillation (AF) treatment decisions in adults with AF.
Study design: Systematic review and meta-analysis.
Eligibility criteria: Eligible randomised controlled trials (RCTs) evaluated digital patient decision-support tools for AF treatment decisions in adults with AF.
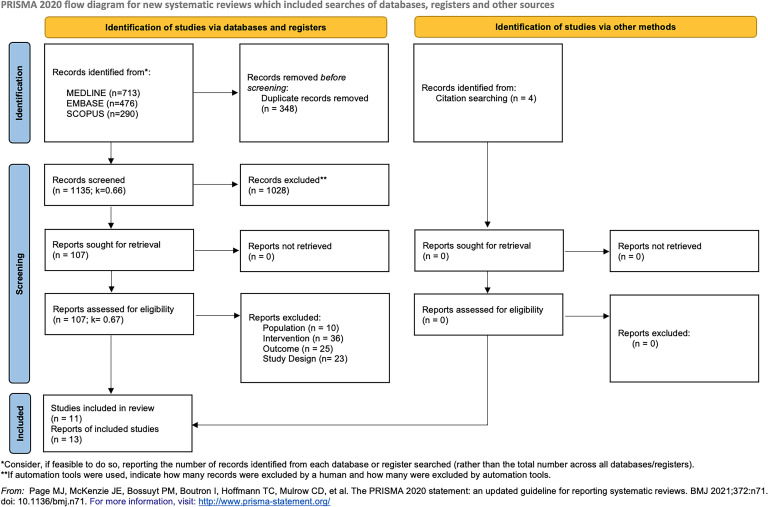
Information sources: We searched MEDLINE, EMBASE and Scopus from 2005 to 2023.Risk-of-bias (RoB) assessment: We assessed RoB using the Cochrane Risk of Bias Tool 2 for RCTs and cluster RCT and the ROBINS-I tool for quasi-experimental studies.
Synthesis of results: We used random effects meta-analysis to synthesise decisional conflict and patient knowledge outcomes reported in RCTs. We performed narrative synthesis for all outcomes. The main outcomes of interest were decisional conflict and patient knowledge.
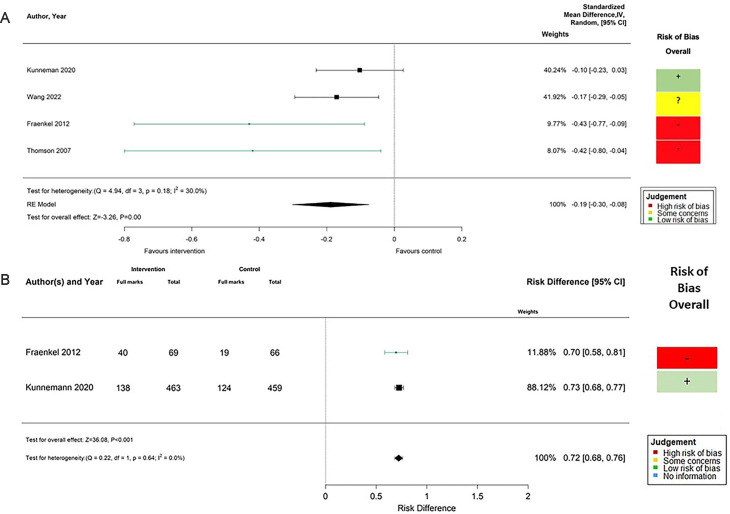
Results: 13 articles, reporting on 11 studies (4 RCTs, 1 cluster RCT and 6 quasi-experimental) met the inclusion criteria. There were 2714 participants across all studies (2372 in RCTs), of which 26% were women and the mean age was 71 years. Socioeconomically disadvantaged groups were poorly represented in the included studies. Seven studies (n=2508) focused on non-valvular AF and the mean CHAD2DS2-VASc across studies was 3.2 and for HAS-BLED 1.9. All tools focused on decisions regarding thromboembolic stroke prevention and most enabled calculation of individualised stroke risk. Tools were heterogeneous in features and functions; four tools were patient decision aids. The readability of content was reported in one study. Meta-analyses showed a reduction in decisional conflict (4 RCTs (n=2167); standardised mean difference -0.19; 95% CI -0.30 to -0.08; p=0.001; I2=26.5%; moderate certainty evidence) corresponding to a decrease in 12.4 units on a scale of 0 to 100 (95% CI -19.5 to -5.2) and improvement in patient knowledge (2 RCTs (n=1057); risk difference 0.72, 95% CI 0.68, 0.76, p<0.001; I2=0%; low certainty evidence) favouring digital patient decision-support tools compared with usual care. Four of the 11 tools were publicly available and 3 had been implemented in healthcare delivery.
Conclusions: In the context of stroke prevention in AF, digital patient decision-support tools likely reduce decisional conflict and may result in little to no change in patient knowledge, compared with usual care. Future studies should leverage digital capabilities for increased personalisation and interactivity of the tools, with better consideration of health literacy and equity aspects. Additional robust trials and implementation studies are warranted.
期刊介绍:
BMJ Evidence-Based Medicine (BMJ EBM) publishes original evidence-based research, insights and opinions on what matters for health care. We focus on the tools, methods, and concepts that are basic and central to practising evidence-based medicine and deliver relevant, trustworthy and impactful evidence.
BMJ EBM is a Plan S compliant Transformative Journal and adheres to the highest possible industry standards for editorial policies and publication ethics.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


