临床 T1b 食管癌的手术和内窥镜治疗。
IF 4.9
1区 医学
Q1 CARDIAC & CARDIOVASCULAR SYSTEMS
Journal of Thoracic and Cardiovascular Surgery
Pub Date : 2025-01-01
DOI:10.1016/j.jtcvs.2024.06.011
引用次数: 0
摘要
目的:侵犯粘膜下层(T1b)的食管癌发生隐匿性淋巴结转移的风险增加。为了避免食管切除术的发病率和恢复期,越来越多的 cT1bN0 肿瘤患者接受了内镜治疗。我们假设肿瘤属性可以预测手术和内镜治疗的上行分期和预后。我们的目的是评估不同cT1bN0肿瘤属性下食管切除术的疗效比较:方法:对2010-2018年间在国家癌症数据库中确诊的临床分期为cT1bN0的食管癌接受内镜治疗或食管切除术的治疗无效患者进行了鉴定。通过逻辑回归评估了与上分期相关的因素。通过对528对倾向匹配配对和加速时间失败模型进行卡普兰-梅耶尔分析评估调整后的生存率,并根据肿瘤属性进行分层:总计发现了 1469 例 cT1bN0 患者,其中 926 例接受了食管切除术,543 例接受了内镜治疗。一般来说,内镜患者年龄较大(中位 71 IQR 63-78 vs.66 IQR 60-72,P1cm,OR=3.19,CI (1.49-6.83),P=0.0028)。倾向匹配的食管切除术患者的总生存率更高(5年68.4%对59.7%,内镜下,PC结论:食管切除术与cT1bN0食管癌生存率的提高有关,但内镜治疗可使肿瘤属性良好的患者获得相似的生存率。值得进一步研究。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Surgical and endoscopic management of clinical T1b esophageal cancer
Objective
Esophageal cancers that invade the submucosa (T1b) have increased risk for occult lymph node metastases. To avoid the morbidity and recovery from esophagectomy, patients with cT1bN0 tumors have been increasingly managed endoscopically. We hypothesized that tumor attributes could predict upstaging and outcome associated with surgical and endoscopic treatment. Our objective was to evaluate the comparative effectiveness of esophagectomy across different cT1bN0 tumor attributes.
Methods
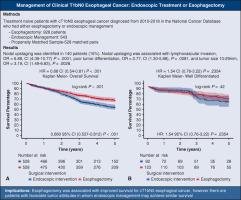
Treatment-naïve patients who underwent endoscopic management or esophagectomy for a clinical stage cT1bN0 esophageal cancer diagnosed between 2010 and 2018 in the National Cancer Database were identified. Factors associated with upstaging were assessed by logistic regression. Adjusted survival was assessed by Kaplan-Meier analysis of 528 propensity-matched pairs and accelerated time failure models, stratified across tumor attributes.
Results
Overall, 1469 patients classified as cT1bN0 were identified; 926 underwent esophagectomy and 543 were managed endoscopically. In general, patients who were managed endoscopically were older (median, 71; interquartile range, 63-78; vs 66; interquartile range, 60-72; P < .0001) with smaller tumors compared with the patients who were managed with esophagectomy. Nodal upstaging was associated with lymphovascular invasion (odds ratio [OR], 6.88; confidence interval [CI], 4.39-10.77; P < .0001), poor tumor differentiation (OR, 2.77; CI, 1.30-5.88; P = .0081), and tumor size >1 cm (OR, 3.19; CI, 1.49-6.83, P = .0028). Overall survival was better among propensity-matched patients who underwent esophagectomy (5-year 68.4% vs 59.7% endoscopic, P < .001). However, accelerated time failure models suggested similar outcomes among patients with well-differentiated tumors managed surgically or endoscopically.
Conclusions
Esophagectomy was associated with improved survival for cT1bN0 esophageal cancer; however, endoscopic treatment may achieve similar survival in patients with favorable tumor attributes. Further study is warranted.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

CiteScore
11.20
自引率
10.00%
发文量
1079
审稿时长
68 days
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


