Toshiaki Iba, Kazuma Yamakawa, Yuki Shiko, Ryo Hisamune, Tomoki Tanigawa, Julie Helms, Jerrold H Levy
{"title":"确定脓毒症所致弥散性血管内凝血抗凝疗法的预后指标。","authors":"Toshiaki Iba, Kazuma Yamakawa, Yuki Shiko, Ryo Hisamune, Tomoki Tanigawa, Julie Helms, Jerrold H Levy","doi":"10.1186/s40560-024-00739-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no reliable indicator that can assess the treatment effect of anticoagulant therapy for sepsis-associated disseminated intravascular coagulation (DIC) in the short term. The aim of this study is to develop and validate a prognostic index identifying 28-day mortality in septic DIC patients treated with antithrombin concentrate after a 3-day treatment.</p><p><strong>Methods: </strong>The cohort for derivation was established utilizing the dataset from post-marketing surveys, while the cohort for validation was acquired from Japan's nationwide sepsis registry data. Through univariate and multivariate analyses, variables that were independently associated with 28-day mortality were identified within the derivation cohort. Risk variables were then assigned a weighted score based on the risk prediction function, leading to the development of a composite index. Subsequently, the area under the receiver operating characteristic curve (AUROC). 28-day survival was compared by Kaplan-Meier analysis.</p><p><strong>Results: </strong>In the derivation cohort, 252 (16.9%) of the 1492 patients deceased within 28 days. Multivariable analysis identified DIC resolution (hazard ratio [HR]: 0.31, 95% confidence interval [CI]: 0.22-0.45, P < 0.0001) and rate of Sequential Organ Failure Assessment (SOFA) score change (HR: 0.42, 95% CI: 0.36-0.50, P < 0.0001) were identified as independent predictors of death. The composite prognostic index (CPI) was constructed as DIC resolution (yes: 1, no: 0) + rate of SOFA score change (Day 0 SOFA score-Day 3 SOFA score/Day 0 SOFA score). When the CPI is higher than 0.19, the patients are judged to survive. Concerning the derivation cohort, AUROC for survival was 0.76. As for the validation cohort, AUROC was 0.71.</p><p><strong>Conclusion: </strong>CPI can predict the 28-day survival of septic patients with DIC who have undergone antithrombin treatment. It is simple and easy to calculate and will be useful in practice.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"12 1","pages":"24"},"PeriodicalIF":4.7000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11194983/pdf/","citationCount":"0","resultStr":"{\"title\":\"Determining prognostic indicator for anticoagulant therapy in sepsis-induced disseminated intravascular coagulation.\",\"authors\":\"Toshiaki Iba, Kazuma Yamakawa, Yuki Shiko, Ryo Hisamune, Tomoki Tanigawa, Julie Helms, Jerrold H Levy\",\"doi\":\"10.1186/s40560-024-00739-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is no reliable indicator that can assess the treatment effect of anticoagulant therapy for sepsis-associated disseminated intravascular coagulation (DIC) in the short term. The aim of this study is to develop and validate a prognostic index identifying 28-day mortality in septic DIC patients treated with antithrombin concentrate after a 3-day treatment.</p><p><strong>Methods: </strong>The cohort for derivation was established utilizing the dataset from post-marketing surveys, while the cohort for validation was acquired from Japan's nationwide sepsis registry data. Through univariate and multivariate analyses, variables that were independently associated with 28-day mortality were identified within the derivation cohort. Risk variables were then assigned a weighted score based on the risk prediction function, leading to the development of a composite index. Subsequently, the area under the receiver operating characteristic curve (AUROC). 28-day survival was compared by Kaplan-Meier analysis.</p><p><strong>Results: </strong>In the derivation cohort, 252 (16.9%) of the 1492 patients deceased within 28 days. Multivariable analysis identified DIC resolution (hazard ratio [HR]: 0.31, 95% confidence interval [CI]: 0.22-0.45, P < 0.0001) and rate of Sequential Organ Failure Assessment (SOFA) score change (HR: 0.42, 95% CI: 0.36-0.50, P < 0.0001) were identified as independent predictors of death. The composite prognostic index (CPI) was constructed as DIC resolution (yes: 1, no: 0) + rate of SOFA score change (Day 0 SOFA score-Day 3 SOFA score/Day 0 SOFA score). When the CPI is higher than 0.19, the patients are judged to survive. Concerning the derivation cohort, AUROC for survival was 0.76. As for the validation cohort, AUROC was 0.71.</p><p><strong>Conclusion: </strong>CPI can predict the 28-day survival of septic patients with DIC who have undergone antithrombin treatment. It is simple and easy to calculate and will be useful in practice.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"12 1\",\"pages\":\"24\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11194983/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-024-00739-x\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-024-00739-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Determining prognostic indicator for anticoagulant therapy in sepsis-induced disseminated intravascular coagulation.
Background: There is no reliable indicator that can assess the treatment effect of anticoagulant therapy for sepsis-associated disseminated intravascular coagulation (DIC) in the short term. The aim of this study is to develop and validate a prognostic index identifying 28-day mortality in septic DIC patients treated with antithrombin concentrate after a 3-day treatment.
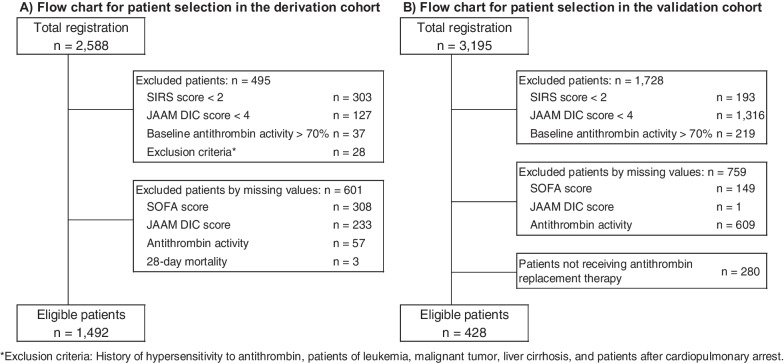
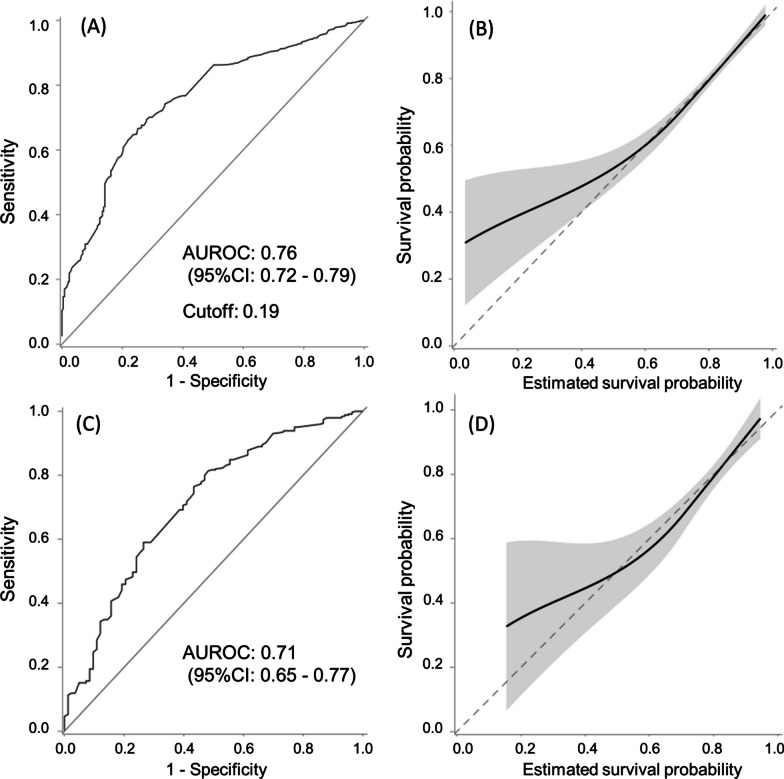
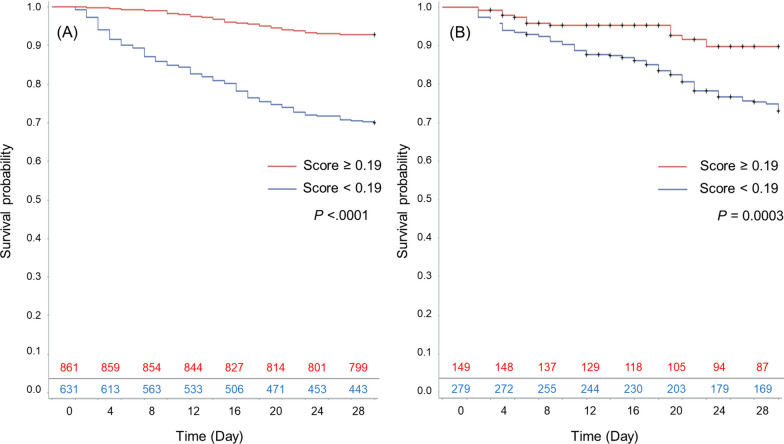
Methods: The cohort for derivation was established utilizing the dataset from post-marketing surveys, while the cohort for validation was acquired from Japan's nationwide sepsis registry data. Through univariate and multivariate analyses, variables that were independently associated with 28-day mortality were identified within the derivation cohort. Risk variables were then assigned a weighted score based on the risk prediction function, leading to the development of a composite index. Subsequently, the area under the receiver operating characteristic curve (AUROC). 28-day survival was compared by Kaplan-Meier analysis.
Results: In the derivation cohort, 252 (16.9%) of the 1492 patients deceased within 28 days. Multivariable analysis identified DIC resolution (hazard ratio [HR]: 0.31, 95% confidence interval [CI]: 0.22-0.45, P < 0.0001) and rate of Sequential Organ Failure Assessment (SOFA) score change (HR: 0.42, 95% CI: 0.36-0.50, P < 0.0001) were identified as independent predictors of death. The composite prognostic index (CPI) was constructed as DIC resolution (yes: 1, no: 0) + rate of SOFA score change (Day 0 SOFA score-Day 3 SOFA score/Day 0 SOFA score). When the CPI is higher than 0.19, the patients are judged to survive. Concerning the derivation cohort, AUROC for survival was 0.76. As for the validation cohort, AUROC was 0.71.
Conclusion: CPI can predict the 28-day survival of septic patients with DIC who have undergone antithrombin treatment. It is simple and easy to calculate and will be useful in practice.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


