Prubpreet Chaggar, Tina Tellum, Lucrezia Viola De Braud, Sarah Annie Solangon, Thulasi Setty, Davor Jurkovic
{"title":"急性腹腔积血后盆腔深部子宫内膜异位症的发展:一项前瞻性超声波研究。","authors":"Prubpreet Chaggar, Tina Tellum, Lucrezia Viola De Braud, Sarah Annie Solangon, Thulasi Setty, Davor Jurkovic","doi":"10.1093/hropen/hoae036","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Is acute haemoperitoneum that is managed conservatively a precursor of deep endometriosis?</p><p><strong>Summary answer: </strong>Our study provides evidence to suggest that acute haemoperitoneum may lead to the development of deep endometriosis in a significant proportion of cases.</p><p><strong>What is known already: </strong>A recent pilot study was the first to suggest that acute haemoperitoneum could be a precursor of deep endometriosis. However, the sample size was small, and the follow-up was not standardized owing to unknown rates of clot absorption and development of endometriosis.</p><p><strong>Study design size duration: </strong>This was a prospective observational cohort study conducted at a single centre over a 31-month period. A required sample size of 30 was calculated using results from a previous study, with a minimum of 15 women each in the groups with and without significant haemoperitoneum (study and control groups, respectively). A total of 59 women were recruited to the study and eight were lost to follow-up. The final sample comprised 51 women, 15 in the study group and 36 in the control group.</p><p><strong>Participants/materials setting methods: </strong>All non-pregnant, premenopausal women aged 18-50 years who consecutively presented to our dedicated gynaecological diagnostic unit with severe acute lower abdominal pain were eligible for this study. We only included women who were clinically stable and were suitable for conservative management. Those with prior history or evidence of endometriosis on their initial ultrasound scan, previous hysterectomy, or bilateral oophorectomy were excluded. Participants had standardized follow-up visits for 6 months, with pelvic ultrasound scans and the British Society of Gynaecological Endoscopy pelvic pain questionnaires completed at each visit. The primary outcome was the sonographically confirmed presence of newly formed endometriosis. Secondary outcomes were the presence and change of pelvic pain symptoms and health-related quality of life (HR-QOL).</p><p><strong>Main results and the role of chance: </strong>After completion of follow-up, 7/15 (47%; 95% CI 21.3-71.4%) women presenting with acute haemoperitoneum (study group) developed sonographic evidence of deep endometriosis, compared to 0/36 (0%; 97.5% CI 0.0-9.7%) women in the control group. A ruptured functional haemorrhagic cyst was the most common cause of haemoperitoneum, occurring in 13/15 cases (87%). The time from the initial event to sonographic evidence of endometriosis varied from 2 to 6 months. The EuroQol visual analogue scores were not significantly different at baseline between the groups that developed and did not develop endometriosis [28 (interquartile range (IQR) 15-40, n = 6) vs 56 (IQR 35-75, n = 44), <i>P </i>=<i> </i>0.09], while the EuroQol-5D values were lower in the endometriosis group [-0.01 (IQR -0.07 to 0.19, n = 6) vs 0.62 (IQR 0.24-0.73, n = 44), <i>P </i>=<i> </i>0.002]. At 6 months, the EuroQol-5D scores were improved in both groups, but remained significantly lower in the endometriosis group compared to the no endometriosis group [0.69 (IQR 0.66-0.80, n = 6) vs 0.85 (IQR 0.76-1.00, n = 44), <i>P </i>=<i> </i>0.03]. There was no clinically relevant difference in the pelvic pain scores at either time point.</p><p><strong>Limitations reasons for caution: </strong>It remains uncertain whether minimal, superficial endometriosis existed at commencement of the study and had a role in the development of deep endometriosis. Although the ultrasound findings were in keeping with deep endometriosis, this was not confirmed histologically. The pelvic pain and HR-QOL findings could have been influenced by the baseline scores being taken when the patient was admitted with acute pain. Also, the sample size was too small to draw reliable conclusions regarding the impact of newly developed endometriosis on QoL.</p><p><strong>Wider implications of the findings: </strong>Our study provides further evidence showing that significant haemoperitoneum may be a precursor of deep endometriosis. Haemodynamically stable women presenting with acute pelvic pain and significant haemoperitoneum should be counselled about the risk of developing deep endometriosis. Interventional studies should be carried out in the future to see whether laparoscopy and pelvic washout could prevent development of deep endometriosis. Preventative strategies, including treatment to suppress ovulation and formation of functional cysts, should be further investigated. This includes the combined and progesterone-only contraceptive pills. Larger future studies are also required to assess women over a longer period of time, with adjustment for confounding factors, to evaluate a possible effect on HR-QOL and pain symptoms.</p><p><strong>Study funding/competing interests: </strong>Funding was obtained from The Gynaecology Ultrasound Centre, London, UK. TT received personal fees from GE, Samsung, Medtronic, and Merck for lectures on ultrasound. TT also received a postdoctoral grant from the South-Eastern Norwegian Health Authority (grant number 2020083).</p><p><strong>Trial registration number: </strong>researchregistry6472.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2024 3","pages":"hoae036"},"PeriodicalIF":11.1000,"publicationDate":"2024-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11189661/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development of deep pelvic endometriosis following acute haemoperitoneum: a prospective ultrasound study.\",\"authors\":\"Prubpreet Chaggar, Tina Tellum, Lucrezia Viola De Braud, Sarah Annie Solangon, Thulasi Setty, Davor Jurkovic\",\"doi\":\"10.1093/hropen/hoae036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>Is acute haemoperitoneum that is managed conservatively a precursor of deep endometriosis?</p><p><strong>Summary answer: </strong>Our study provides evidence to suggest that acute haemoperitoneum may lead to the development of deep endometriosis in a significant proportion of cases.</p><p><strong>What is known already: </strong>A recent pilot study was the first to suggest that acute haemoperitoneum could be a precursor of deep endometriosis. However, the sample size was small, and the follow-up was not standardized owing to unknown rates of clot absorption and development of endometriosis.</p><p><strong>Study design size duration: </strong>This was a prospective observational cohort study conducted at a single centre over a 31-month period. A required sample size of 30 was calculated using results from a previous study, with a minimum of 15 women each in the groups with and without significant haemoperitoneum (study and control groups, respectively). A total of 59 women were recruited to the study and eight were lost to follow-up. The final sample comprised 51 women, 15 in the study group and 36 in the control group.</p><p><strong>Participants/materials setting methods: </strong>All non-pregnant, premenopausal women aged 18-50 years who consecutively presented to our dedicated gynaecological diagnostic unit with severe acute lower abdominal pain were eligible for this study. We only included women who were clinically stable and were suitable for conservative management. Those with prior history or evidence of endometriosis on their initial ultrasound scan, previous hysterectomy, or bilateral oophorectomy were excluded. Participants had standardized follow-up visits for 6 months, with pelvic ultrasound scans and the British Society of Gynaecological Endoscopy pelvic pain questionnaires completed at each visit. The primary outcome was the sonographically confirmed presence of newly formed endometriosis. Secondary outcomes were the presence and change of pelvic pain symptoms and health-related quality of life (HR-QOL).</p><p><strong>Main results and the role of chance: </strong>After completion of follow-up, 7/15 (47%; 95% CI 21.3-71.4%) women presenting with acute haemoperitoneum (study group) developed sonographic evidence of deep endometriosis, compared to 0/36 (0%; 97.5% CI 0.0-9.7%) women in the control group. A ruptured functional haemorrhagic cyst was the most common cause of haemoperitoneum, occurring in 13/15 cases (87%). The time from the initial event to sonographic evidence of endometriosis varied from 2 to 6 months. The EuroQol visual analogue scores were not significantly different at baseline between the groups that developed and did not develop endometriosis [28 (interquartile range (IQR) 15-40, n = 6) vs 56 (IQR 35-75, n = 44), <i>P </i>=<i> </i>0.09], while the EuroQol-5D values were lower in the endometriosis group [-0.01 (IQR -0.07 to 0.19, n = 6) vs 0.62 (IQR 0.24-0.73, n = 44), <i>P </i>=<i> </i>0.002]. At 6 months, the EuroQol-5D scores were improved in both groups, but remained significantly lower in the endometriosis group compared to the no endometriosis group [0.69 (IQR 0.66-0.80, n = 6) vs 0.85 (IQR 0.76-1.00, n = 44), <i>P </i>=<i> </i>0.03]. There was no clinically relevant difference in the pelvic pain scores at either time point.</p><p><strong>Limitations reasons for caution: </strong>It remains uncertain whether minimal, superficial endometriosis existed at commencement of the study and had a role in the development of deep endometriosis. Although the ultrasound findings were in keeping with deep endometriosis, this was not confirmed histologically. The pelvic pain and HR-QOL findings could have been influenced by the baseline scores being taken when the patient was admitted with acute pain. Also, the sample size was too small to draw reliable conclusions regarding the impact of newly developed endometriosis on QoL.</p><p><strong>Wider implications of the findings: </strong>Our study provides further evidence showing that significant haemoperitoneum may be a precursor of deep endometriosis. Haemodynamically stable women presenting with acute pelvic pain and significant haemoperitoneum should be counselled about the risk of developing deep endometriosis. Interventional studies should be carried out in the future to see whether laparoscopy and pelvic washout could prevent development of deep endometriosis. Preventative strategies, including treatment to suppress ovulation and formation of functional cysts, should be further investigated. This includes the combined and progesterone-only contraceptive pills. Larger future studies are also required to assess women over a longer period of time, with adjustment for confounding factors, to evaluate a possible effect on HR-QOL and pain symptoms.</p><p><strong>Study funding/competing interests: </strong>Funding was obtained from The Gynaecology Ultrasound Centre, London, UK. TT received personal fees from GE, Samsung, Medtronic, and Merck for lectures on ultrasound. TT also received a postdoctoral grant from the South-Eastern Norwegian Health Authority (grant number 2020083).</p><p><strong>Trial registration number: </strong>researchregistry6472.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2024 3\",\"pages\":\"hoae036\"},\"PeriodicalIF\":11.1000,\"publicationDate\":\"2024-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11189661/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoae036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoae036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Development of deep pelvic endometriosis following acute haemoperitoneum: a prospective ultrasound study.
Study question: Is acute haemoperitoneum that is managed conservatively a precursor of deep endometriosis?
Summary answer: Our study provides evidence to suggest that acute haemoperitoneum may lead to the development of deep endometriosis in a significant proportion of cases.
What is known already: A recent pilot study was the first to suggest that acute haemoperitoneum could be a precursor of deep endometriosis. However, the sample size was small, and the follow-up was not standardized owing to unknown rates of clot absorption and development of endometriosis.
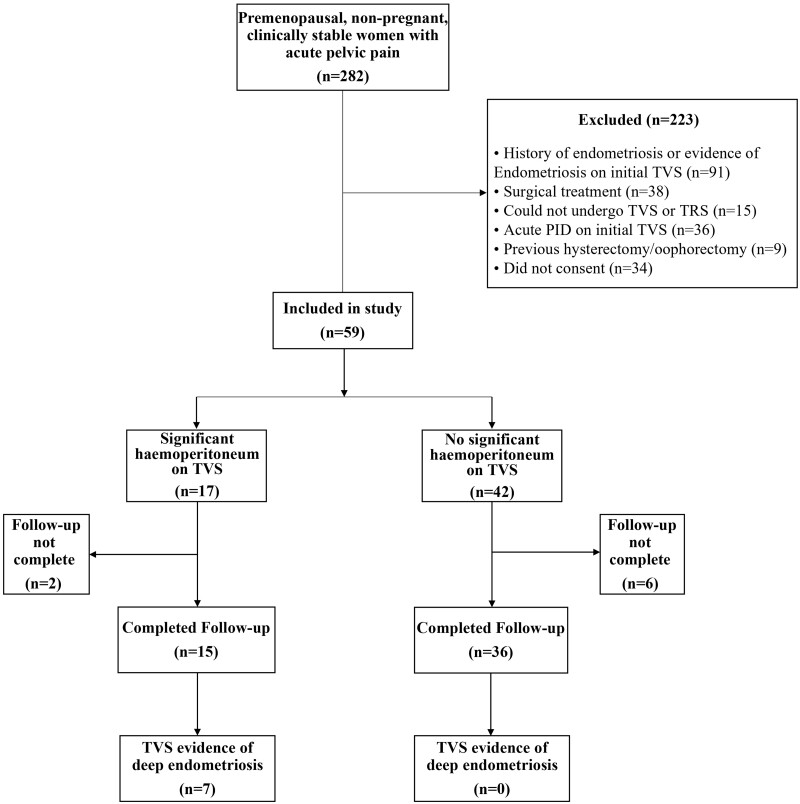
Study design size duration: This was a prospective observational cohort study conducted at a single centre over a 31-month period. A required sample size of 30 was calculated using results from a previous study, with a minimum of 15 women each in the groups with and without significant haemoperitoneum (study and control groups, respectively). A total of 59 women were recruited to the study and eight were lost to follow-up. The final sample comprised 51 women, 15 in the study group and 36 in the control group.
Participants/materials setting methods: All non-pregnant, premenopausal women aged 18-50 years who consecutively presented to our dedicated gynaecological diagnostic unit with severe acute lower abdominal pain were eligible for this study. We only included women who were clinically stable and were suitable for conservative management. Those with prior history or evidence of endometriosis on their initial ultrasound scan, previous hysterectomy, or bilateral oophorectomy were excluded. Participants had standardized follow-up visits for 6 months, with pelvic ultrasound scans and the British Society of Gynaecological Endoscopy pelvic pain questionnaires completed at each visit. The primary outcome was the sonographically confirmed presence of newly formed endometriosis. Secondary outcomes were the presence and change of pelvic pain symptoms and health-related quality of life (HR-QOL).
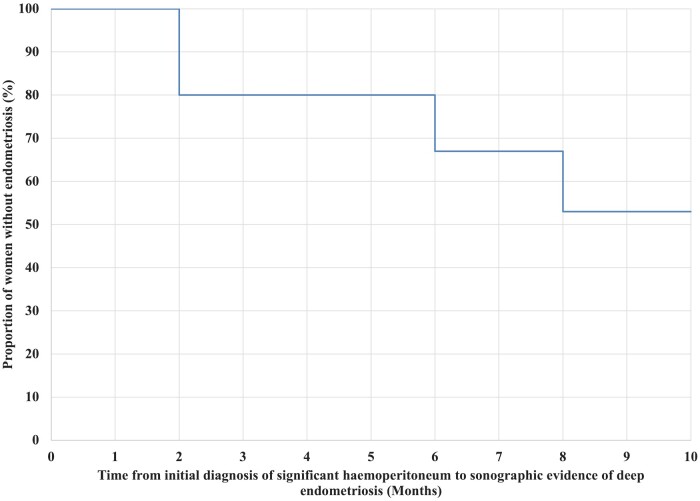
Main results and the role of chance: After completion of follow-up, 7/15 (47%; 95% CI 21.3-71.4%) women presenting with acute haemoperitoneum (study group) developed sonographic evidence of deep endometriosis, compared to 0/36 (0%; 97.5% CI 0.0-9.7%) women in the control group. A ruptured functional haemorrhagic cyst was the most common cause of haemoperitoneum, occurring in 13/15 cases (87%). The time from the initial event to sonographic evidence of endometriosis varied from 2 to 6 months. The EuroQol visual analogue scores were not significantly different at baseline between the groups that developed and did not develop endometriosis [28 (interquartile range (IQR) 15-40, n = 6) vs 56 (IQR 35-75, n = 44), P =0.09], while the EuroQol-5D values were lower in the endometriosis group [-0.01 (IQR -0.07 to 0.19, n = 6) vs 0.62 (IQR 0.24-0.73, n = 44), P =0.002]. At 6 months, the EuroQol-5D scores were improved in both groups, but remained significantly lower in the endometriosis group compared to the no endometriosis group [0.69 (IQR 0.66-0.80, n = 6) vs 0.85 (IQR 0.76-1.00, n = 44), P =0.03]. There was no clinically relevant difference in the pelvic pain scores at either time point.
Limitations reasons for caution: It remains uncertain whether minimal, superficial endometriosis existed at commencement of the study and had a role in the development of deep endometriosis. Although the ultrasound findings were in keeping with deep endometriosis, this was not confirmed histologically. The pelvic pain and HR-QOL findings could have been influenced by the baseline scores being taken when the patient was admitted with acute pain. Also, the sample size was too small to draw reliable conclusions regarding the impact of newly developed endometriosis on QoL.
Wider implications of the findings: Our study provides further evidence showing that significant haemoperitoneum may be a precursor of deep endometriosis. Haemodynamically stable women presenting with acute pelvic pain and significant haemoperitoneum should be counselled about the risk of developing deep endometriosis. Interventional studies should be carried out in the future to see whether laparoscopy and pelvic washout could prevent development of deep endometriosis. Preventative strategies, including treatment to suppress ovulation and formation of functional cysts, should be further investigated. This includes the combined and progesterone-only contraceptive pills. Larger future studies are also required to assess women over a longer period of time, with adjustment for confounding factors, to evaluate a possible effect on HR-QOL and pain symptoms.
Study funding/competing interests: Funding was obtained from The Gynaecology Ultrasound Centre, London, UK. TT received personal fees from GE, Samsung, Medtronic, and Merck for lectures on ultrasound. TT also received a postdoctoral grant from the South-Eastern Norwegian Health Authority (grant number 2020083).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


