Zhiwei Lin , Chanjuan Chen , Shengyuan Xie , Lei Chen , Yusheng Yao , Bin Qian
{"title":"全身利多卡因与直立肌脊柱平面阻滞在改善腹腔镜胆囊切除术后恢复质量方面的比较:随机对照试验","authors":"Zhiwei Lin , Chanjuan Chen , Shengyuan Xie , Lei Chen , Yusheng Yao , Bin Qian","doi":"10.1016/j.jclinane.2024.111528","DOIUrl":null,"url":null,"abstract":"<div><h3>Study objective</h3><p>To compare intravenous lidocaine, ultrasound-guided erector spinae plane block (ESPB), and placebo on the quality of recovery and analgesia after laparoscopic cholecystectomy.</p></div><div><h3>Design</h3><p>A prospective, triple-arm, double-blind, randomized, placebo-controlled non-inferiority trial.</p></div><div><h3>Setting</h3><p>A single tertiary academic medical center.</p></div><div><h3>Patients</h3><p>126 adults aged 18–65 years undergoing elective laparoscopic cholecystectomy.</p></div><div><h3>Interventions</h3><p>Patients were randomly allocated to one of three groups: intravenous lidocaine infusion (1.5 mg/kg bolus followed by 2 mg/kg/h) plus bilateral ESPB with saline (25 mL per side); bilateral ESPB with 0.25% ropivacaine (25 ml per side) plus placebo infusion; or bilateral ESPB with saline (25 ml per side) plus placebo infusion.</p></div><div><h3>Measurements</h3><p>The primary outcome was the 24-h postoperative Quality of Recovery-15 (QoR-15) score. The non-inferiority of lidocaine versus ESPB was assessed with a margin of −6 points and 97.5% confidence interval (CI). Secondary outcomes included 24-h area under the curve (AUC) for pain scores, morphine consumption, and adverse events.</p></div><div><h3>Main results</h3><p>124 patients completed the study. Median (IQR) 24-h QoR-15 scores were 123 (117–127) for lidocaine, 124 (119–126) for ESPB, and 112 (108–117) for placebo. Lidocaine was non-inferior to ESPB (median difference –1, 97.5% CI: −4 to ∞). Both lidocaine (median difference 9, 95% CI: 6–12, <em>P</em> < 0.001) and ESPB (median difference 10, 95% CI: 7–13, <em>P</em> < 0.001) were superior to placebo. AUC for pain scores and morphine use were lower with lidocaine and ESPB versus placebo (<em>P</em> < 0.001 for all), with no significant differences between lidocaine and ESPB. One ESPB patient reported a transient metallic taste; no other block-related complications occurred.</p></div><div><h3>Conclusions</h3><p>For patients undergoing laparoscopic cholecystectomy, intravenous lidocaine provides a non-inferior quality of recovery compared to ESPB without requiring specialized regional anesthesia procedures. Lidocaine may offer a practical and accessible alternative within multimodal analgesia pathways.</p></div>","PeriodicalId":15506,"journal":{"name":"Journal of Clinical Anesthesia","volume":null,"pages":null},"PeriodicalIF":5.0000,"publicationDate":"2024-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Systemic lidocaine versus erector spinae plane block for improving quality of recovery after laparoscopic cholecystectomy: A randomized controlled trial\",\"authors\":\"Zhiwei Lin , Chanjuan Chen , Shengyuan Xie , Lei Chen , Yusheng Yao , Bin Qian\",\"doi\":\"10.1016/j.jclinane.2024.111528\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Study objective</h3><p>To compare intravenous lidocaine, ultrasound-guided erector spinae plane block (ESPB), and placebo on the quality of recovery and analgesia after laparoscopic cholecystectomy.</p></div><div><h3>Design</h3><p>A prospective, triple-arm, double-blind, randomized, placebo-controlled non-inferiority trial.</p></div><div><h3>Setting</h3><p>A single tertiary academic medical center.</p></div><div><h3>Patients</h3><p>126 adults aged 18–65 years undergoing elective laparoscopic cholecystectomy.</p></div><div><h3>Interventions</h3><p>Patients were randomly allocated to one of three groups: intravenous lidocaine infusion (1.5 mg/kg bolus followed by 2 mg/kg/h) plus bilateral ESPB with saline (25 mL per side); bilateral ESPB with 0.25% ropivacaine (25 ml per side) plus placebo infusion; or bilateral ESPB with saline (25 ml per side) plus placebo infusion.</p></div><div><h3>Measurements</h3><p>The primary outcome was the 24-h postoperative Quality of Recovery-15 (QoR-15) score. The non-inferiority of lidocaine versus ESPB was assessed with a margin of −6 points and 97.5% confidence interval (CI). Secondary outcomes included 24-h area under the curve (AUC) for pain scores, morphine consumption, and adverse events.</p></div><div><h3>Main results</h3><p>124 patients completed the study. Median (IQR) 24-h QoR-15 scores were 123 (117–127) for lidocaine, 124 (119–126) for ESPB, and 112 (108–117) for placebo. Lidocaine was non-inferior to ESPB (median difference –1, 97.5% CI: −4 to ∞). Both lidocaine (median difference 9, 95% CI: 6–12, <em>P</em> < 0.001) and ESPB (median difference 10, 95% CI: 7–13, <em>P</em> < 0.001) were superior to placebo. AUC for pain scores and morphine use were lower with lidocaine and ESPB versus placebo (<em>P</em> < 0.001 for all), with no significant differences between lidocaine and ESPB. One ESPB patient reported a transient metallic taste; no other block-related complications occurred.</p></div><div><h3>Conclusions</h3><p>For patients undergoing laparoscopic cholecystectomy, intravenous lidocaine provides a non-inferior quality of recovery compared to ESPB without requiring specialized regional anesthesia procedures. Lidocaine may offer a practical and accessible alternative within multimodal analgesia pathways.</p></div>\",\"PeriodicalId\":15506,\"journal\":{\"name\":\"Journal of Clinical Anesthesia\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Anesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0952818024001570\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0952818024001570","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
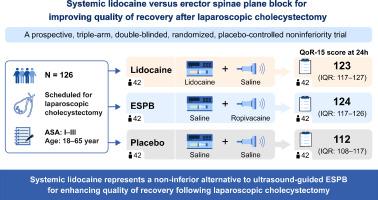
Systemic lidocaine versus erector spinae plane block for improving quality of recovery after laparoscopic cholecystectomy: A randomized controlled trial
Study objective
To compare intravenous lidocaine, ultrasound-guided erector spinae plane block (ESPB), and placebo on the quality of recovery and analgesia after laparoscopic cholecystectomy.
Design
A prospective, triple-arm, double-blind, randomized, placebo-controlled non-inferiority trial.
Setting
A single tertiary academic medical center.
Patients
126 adults aged 18–65 years undergoing elective laparoscopic cholecystectomy.
Interventions
Patients were randomly allocated to one of three groups: intravenous lidocaine infusion (1.5 mg/kg bolus followed by 2 mg/kg/h) plus bilateral ESPB with saline (25 mL per side); bilateral ESPB with 0.25% ropivacaine (25 ml per side) plus placebo infusion; or bilateral ESPB with saline (25 ml per side) plus placebo infusion.
Measurements
The primary outcome was the 24-h postoperative Quality of Recovery-15 (QoR-15) score. The non-inferiority of lidocaine versus ESPB was assessed with a margin of −6 points and 97.5% confidence interval (CI). Secondary outcomes included 24-h area under the curve (AUC) for pain scores, morphine consumption, and adverse events.
Main results
124 patients completed the study. Median (IQR) 24-h QoR-15 scores were 123 (117–127) for lidocaine, 124 (119–126) for ESPB, and 112 (108–117) for placebo. Lidocaine was non-inferior to ESPB (median difference –1, 97.5% CI: −4 to ∞). Both lidocaine (median difference 9, 95% CI: 6–12, P < 0.001) and ESPB (median difference 10, 95% CI: 7–13, P < 0.001) were superior to placebo. AUC for pain scores and morphine use were lower with lidocaine and ESPB versus placebo (P < 0.001 for all), with no significant differences between lidocaine and ESPB. One ESPB patient reported a transient metallic taste; no other block-related complications occurred.
Conclusions
For patients undergoing laparoscopic cholecystectomy, intravenous lidocaine provides a non-inferior quality of recovery compared to ESPB without requiring specialized regional anesthesia procedures. Lidocaine may offer a practical and accessible alternative within multimodal analgesia pathways.
期刊介绍:
The Journal of Clinical Anesthesia (JCA) addresses all aspects of anesthesia practice, including anesthetic administration, pharmacokinetics, preoperative and postoperative considerations, coexisting disease and other complicating factors, cost issues, and similar concerns anesthesiologists contend with daily. Exceptionally high standards of presentation and accuracy are maintained.
The core of the journal is original contributions on subjects relevant to clinical practice, and rigorously peer-reviewed. Highly respected international experts have joined together to form the Editorial Board, sharing their years of experience and clinical expertise. Specialized section editors cover the various subspecialties within the field. To keep your practical clinical skills current, the journal bridges the gap between the laboratory and the clinical practice of anesthesiology and critical care to clarify how new insights can improve daily practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


