Hannes Gatterer, Francisco C Villafuerte, Silvia Ulrich, Sanjeeb S Bhandari, Linda E Keyes, Martin Burtscher
{"title":"高原病。","authors":"Hannes Gatterer, Francisco C Villafuerte, Silvia Ulrich, Sanjeeb S Bhandari, Linda E Keyes, Martin Burtscher","doi":"10.1038/s41572-024-00526-w","DOIUrl":null,"url":null,"abstract":"<p><p>Millions of people visit high-altitude regions annually and more than 80 million live permanently above 2,500 m. Acute high-altitude exposure can trigger high-altitude illnesses (HAIs), including acute mountain sickness (AMS), high-altitude cerebral oedema (HACE) and high-altitude pulmonary oedema (HAPE). Chronic mountain sickness (CMS) can affect high-altitude resident populations worldwide. The prevalence of acute HAIs varies according to acclimatization status, rate of ascent and individual susceptibility. AMS, characterized by headache, nausea, dizziness and fatigue, is usually benign and self-limiting, and has been linked to hypoxia-induced cerebral blood volume increases, inflammation and related trigeminovascular system activation. Disruption of the blood-brain barrier leads to HACE, characterized by altered mental status and ataxia, and increased pulmonary capillary pressure, and related stress failure induces HAPE, characterized by dyspnoea, cough and exercise intolerance. Both conditions are progressive and life-threatening, requiring immediate medical intervention. Treatment includes supplemental oxygen and descent with appropriate pharmacological therapy. Preventive measures include slow ascent, pre-acclimatization and, in some instances, medications. CMS is characterized by excessive erythrocytosis and related clinical symptoms. In severe CMS, temporary or permanent relocation to low altitude is recommended. Future research should focus on more objective diagnostic tools to enable prompt treatment, improved identification of individual susceptibilities and effective acclimatization and prevention options.</p>","PeriodicalId":18910,"journal":{"name":"Nature Reviews Disease Primers","volume":"10 1","pages":"43"},"PeriodicalIF":76.9000,"publicationDate":"2024-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Altitude illnesses.\",\"authors\":\"Hannes Gatterer, Francisco C Villafuerte, Silvia Ulrich, Sanjeeb S Bhandari, Linda E Keyes, Martin Burtscher\",\"doi\":\"10.1038/s41572-024-00526-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Millions of people visit high-altitude regions annually and more than 80 million live permanently above 2,500 m. Acute high-altitude exposure can trigger high-altitude illnesses (HAIs), including acute mountain sickness (AMS), high-altitude cerebral oedema (HACE) and high-altitude pulmonary oedema (HAPE). Chronic mountain sickness (CMS) can affect high-altitude resident populations worldwide. The prevalence of acute HAIs varies according to acclimatization status, rate of ascent and individual susceptibility. AMS, characterized by headache, nausea, dizziness and fatigue, is usually benign and self-limiting, and has been linked to hypoxia-induced cerebral blood volume increases, inflammation and related trigeminovascular system activation. Disruption of the blood-brain barrier leads to HACE, characterized by altered mental status and ataxia, and increased pulmonary capillary pressure, and related stress failure induces HAPE, characterized by dyspnoea, cough and exercise intolerance. Both conditions are progressive and life-threatening, requiring immediate medical intervention. Treatment includes supplemental oxygen and descent with appropriate pharmacological therapy. Preventive measures include slow ascent, pre-acclimatization and, in some instances, medications. CMS is characterized by excessive erythrocytosis and related clinical symptoms. In severe CMS, temporary or permanent relocation to low altitude is recommended. Future research should focus on more objective diagnostic tools to enable prompt treatment, improved identification of individual susceptibilities and effective acclimatization and prevention options.</p>\",\"PeriodicalId\":18910,\"journal\":{\"name\":\"Nature Reviews Disease Primers\",\"volume\":\"10 1\",\"pages\":\"43\"},\"PeriodicalIF\":76.9000,\"publicationDate\":\"2024-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Reviews Disease Primers\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41572-024-00526-w\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Reviews Disease Primers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41572-024-00526-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
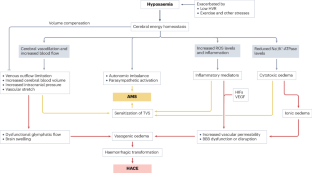
Millions of people visit high-altitude regions annually and more than 80 million live permanently above 2,500 m. Acute high-altitude exposure can trigger high-altitude illnesses (HAIs), including acute mountain sickness (AMS), high-altitude cerebral oedema (HACE) and high-altitude pulmonary oedema (HAPE). Chronic mountain sickness (CMS) can affect high-altitude resident populations worldwide. The prevalence of acute HAIs varies according to acclimatization status, rate of ascent and individual susceptibility. AMS, characterized by headache, nausea, dizziness and fatigue, is usually benign and self-limiting, and has been linked to hypoxia-induced cerebral blood volume increases, inflammation and related trigeminovascular system activation. Disruption of the blood-brain barrier leads to HACE, characterized by altered mental status and ataxia, and increased pulmonary capillary pressure, and related stress failure induces HAPE, characterized by dyspnoea, cough and exercise intolerance. Both conditions are progressive and life-threatening, requiring immediate medical intervention. Treatment includes supplemental oxygen and descent with appropriate pharmacological therapy. Preventive measures include slow ascent, pre-acclimatization and, in some instances, medications. CMS is characterized by excessive erythrocytosis and related clinical symptoms. In severe CMS, temporary or permanent relocation to low altitude is recommended. Future research should focus on more objective diagnostic tools to enable prompt treatment, improved identification of individual susceptibilities and effective acclimatization and prevention options.
期刊介绍:
Nature Reviews Disease Primers, a part of the Nature Reviews journal portfolio, features sections on epidemiology, mechanisms, diagnosis, management, and patient quality of life. The editorial team commissions top researchers — comprising basic scientists and clinical researchers — to write the Primers, which are designed for use by early career researchers, medical students and principal investigators. Each Primer concludes with an Outlook section, highlighting future research directions. Covered medical specialties include Cardiology, Dermatology, Ear, Nose and Throat, Emergency Medicine, Endocrinology, Gastroenterology, Genetic Conditions, Gynaecology and Obstetrics, Hepatology, Haematology, Infectious Diseases, Maxillofacial and Oral Medicine, Nephrology, Neurology, Nutrition, Oncology, Ophthalmology, Orthopaedics, Psychiatry, Respiratory Medicine, Rheumatology, Sleep Medicine, and Urology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


