{"title":"肝细胞癌在诊断时直接侵犯胃部","authors":"Pei-Jung Chen, Tyng-Yuan Jang","doi":"10.1002/aid2.13384","DOIUrl":null,"url":null,"abstract":"<p>A 48-year-old man with melena was admitted to our hospital for 1 month. The patient denied any history of systemic disease, and had no history of cirrhosis, esophageal varices or thrombocytopenia. He sometimes drinks but did not achieve the criteria of alcoholism (≥20 g daily). Upper endoscopy revealed an ulcerative mass in the gastric body. The patient underwent endoscopic biopsy (Figure 1A). Computed tomography (CT) revealed tumors in the bilateral hepatic lobes without vascular invasion or extra-hepatic metastasis; and the left-lobe tumor directly invaded the stomach (Figure 1B). Laboratory tests showed 5 g/dL hemoglobin, 599 × 10<sup>3</sup>/μL platelet count, and 2839.04 IU/mL alpha-fetoprotein levels. Hepatitis B surface antigen, HBV DNA and antibodies to hepatitis C virus were negative. Anti-hepatitis B core antibody IgG was positive. Pathological examination of the gastric tumor revealed metastatic HCC (Figure 1C). Immunohistochemical analysis of the tumor tissue showed negative expression for CK7, CK20, and CDX-2, but positive expression for hepatocyte paraffin-1 (Hep par-1) (Figure 1D) and glypican-3 (GPC-3). After the confirmation of metastatic HCC, he received transarterial chemoembolization and lenvatinib therapy but died several months later owing to tumor progression.</p><p>The most common extrahepatic metastatic sites are the lungs, bones, and lymph nodes. In contrast, HCC metastases to the gastrointestinal (GI) tract are rare, and the mortality rate is high. After diagnosis of GI metastases, the average remaining lifespan is approximately 7.3 months.<span><sup>1</sup></span> Sohn et al. reported the earliest case of HCC metastasis to the GI tract in 1965. The tumor was approximately of 6 cm, and located in the left hepatic lobe with portal vein invasion, and metastasized to the esophagus.<span><sup>2</sup></span> Shiota et al. reported the first case of HCC with stomach invasion in which the tumor was located in both the right and left hepatic lobe.<span><sup>3</sup></span></p><p>A systematic review published by Urhut et al. in 2022 included 192 patients, 87.3% of whom were male.<span><sup>1</sup></span> According to the report, the most common GI tract metastases were in the stomach (27.9%) and duodenum (27.9%). Most routes of metastasis were direct invasion and hematogenous metastasis. Therefore, risk factors for HCC with GI tract metastases included growth mode, tumor size, tumor localization, and portal vein invasion. Because of their close anatomical location, tumors located on the right side of the liver are more likely to invade the duodenum, whereas tumors located on the left side of the liver are more likely to invade the stomach.<span><sup>1</sup></span> Symptoms of HCC with GI invasion include GI bleeding, anemia, abdominal pain, palpable masses, nausea, and vomiting. Esophagogastroduodenoscopy and abdominal contrast-CT are the most useful diagnostic tools. Histological evidence can help diagnose HCC with GI invasion and differentiate between HCC and GI cancer. Immunohistochemical evidence for diagnosing HCC included Hep par-1, arginase-1, GPC-3, and polyclonal carcinoembryonic antigen.<span><sup>4</sup></span> In addition, hepatoid adenocarcinoma, a rare extrahepatic adenocarcinoma, was a differential diagnosis of gastric tumor with high AFP.<span><sup>5</sup></span></p><p>In conclusion, HCC with GI tract invasion as the first presentation is rare. However, HCC with GI metastasis should be considered when HCC patients present with GI bleeding and anemia. Endoscopy is the gold standard method for diagnosing HCC with GI tract invasion. Although many treatment strategies are available for HCC, the prognosis of patients with liver cancer complicated by GI metastases is poor.</p><p>The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 2","pages":"110-111"},"PeriodicalIF":0.4000,"publicationDate":"2023-12-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13384","citationCount":"0","resultStr":"{\"title\":\"Hepatocellular carcinoma directly invaded the stomach at the time of diagnosis\",\"authors\":\"Pei-Jung Chen, Tyng-Yuan Jang\",\"doi\":\"10.1002/aid2.13384\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 48-year-old man with melena was admitted to our hospital for 1 month. The patient denied any history of systemic disease, and had no history of cirrhosis, esophageal varices or thrombocytopenia. He sometimes drinks but did not achieve the criteria of alcoholism (≥20 g daily). Upper endoscopy revealed an ulcerative mass in the gastric body. The patient underwent endoscopic biopsy (Figure 1A). Computed tomography (CT) revealed tumors in the bilateral hepatic lobes without vascular invasion or extra-hepatic metastasis; and the left-lobe tumor directly invaded the stomach (Figure 1B). Laboratory tests showed 5 g/dL hemoglobin, 599 × 10<sup>3</sup>/μL platelet count, and 2839.04 IU/mL alpha-fetoprotein levels. Hepatitis B surface antigen, HBV DNA and antibodies to hepatitis C virus were negative. Anti-hepatitis B core antibody IgG was positive. Pathological examination of the gastric tumor revealed metastatic HCC (Figure 1C). Immunohistochemical analysis of the tumor tissue showed negative expression for CK7, CK20, and CDX-2, but positive expression for hepatocyte paraffin-1 (Hep par-1) (Figure 1D) and glypican-3 (GPC-3). After the confirmation of metastatic HCC, he received transarterial chemoembolization and lenvatinib therapy but died several months later owing to tumor progression.</p><p>The most common extrahepatic metastatic sites are the lungs, bones, and lymph nodes. In contrast, HCC metastases to the gastrointestinal (GI) tract are rare, and the mortality rate is high. After diagnosis of GI metastases, the average remaining lifespan is approximately 7.3 months.<span><sup>1</sup></span> Sohn et al. reported the earliest case of HCC metastasis to the GI tract in 1965. The tumor was approximately of 6 cm, and located in the left hepatic lobe with portal vein invasion, and metastasized to the esophagus.<span><sup>2</sup></span> Shiota et al. reported the first case of HCC with stomach invasion in which the tumor was located in both the right and left hepatic lobe.<span><sup>3</sup></span></p><p>A systematic review published by Urhut et al. in 2022 included 192 patients, 87.3% of whom were male.<span><sup>1</sup></span> According to the report, the most common GI tract metastases were in the stomach (27.9%) and duodenum (27.9%). Most routes of metastasis were direct invasion and hematogenous metastasis. Therefore, risk factors for HCC with GI tract metastases included growth mode, tumor size, tumor localization, and portal vein invasion. Because of their close anatomical location, tumors located on the right side of the liver are more likely to invade the duodenum, whereas tumors located on the left side of the liver are more likely to invade the stomach.<span><sup>1</sup></span> Symptoms of HCC with GI invasion include GI bleeding, anemia, abdominal pain, palpable masses, nausea, and vomiting. Esophagogastroduodenoscopy and abdominal contrast-CT are the most useful diagnostic tools. Histological evidence can help diagnose HCC with GI invasion and differentiate between HCC and GI cancer. Immunohistochemical evidence for diagnosing HCC included Hep par-1, arginase-1, GPC-3, and polyclonal carcinoembryonic antigen.<span><sup>4</sup></span> In addition, hepatoid adenocarcinoma, a rare extrahepatic adenocarcinoma, was a differential diagnosis of gastric tumor with high AFP.<span><sup>5</sup></span></p><p>In conclusion, HCC with GI tract invasion as the first presentation is rare. However, HCC with GI metastasis should be considered when HCC patients present with GI bleeding and anemia. Endoscopy is the gold standard method for diagnosing HCC with GI tract invasion. Although many treatment strategies are available for HCC, the prognosis of patients with liver cancer complicated by GI metastases is poor.</p><p>The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"11 2\",\"pages\":\"110-111\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2023-12-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13384\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13384\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13384","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Hepatocellular carcinoma directly invaded the stomach at the time of diagnosis
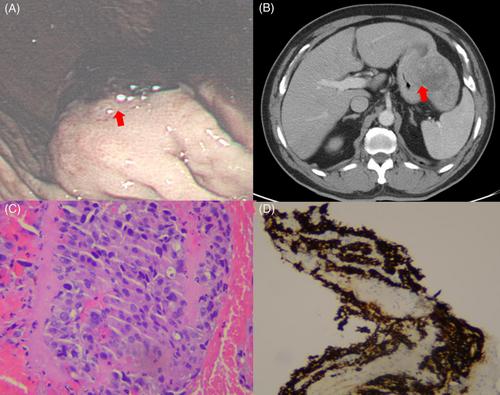
A 48-year-old man with melena was admitted to our hospital for 1 month. The patient denied any history of systemic disease, and had no history of cirrhosis, esophageal varices or thrombocytopenia. He sometimes drinks but did not achieve the criteria of alcoholism (≥20 g daily). Upper endoscopy revealed an ulcerative mass in the gastric body. The patient underwent endoscopic biopsy (Figure 1A). Computed tomography (CT) revealed tumors in the bilateral hepatic lobes without vascular invasion or extra-hepatic metastasis; and the left-lobe tumor directly invaded the stomach (Figure 1B). Laboratory tests showed 5 g/dL hemoglobin, 599 × 103/μL platelet count, and 2839.04 IU/mL alpha-fetoprotein levels. Hepatitis B surface antigen, HBV DNA and antibodies to hepatitis C virus were negative. Anti-hepatitis B core antibody IgG was positive. Pathological examination of the gastric tumor revealed metastatic HCC (Figure 1C). Immunohistochemical analysis of the tumor tissue showed negative expression for CK7, CK20, and CDX-2, but positive expression for hepatocyte paraffin-1 (Hep par-1) (Figure 1D) and glypican-3 (GPC-3). After the confirmation of metastatic HCC, he received transarterial chemoembolization and lenvatinib therapy but died several months later owing to tumor progression.
The most common extrahepatic metastatic sites are the lungs, bones, and lymph nodes. In contrast, HCC metastases to the gastrointestinal (GI) tract are rare, and the mortality rate is high. After diagnosis of GI metastases, the average remaining lifespan is approximately 7.3 months.1 Sohn et al. reported the earliest case of HCC metastasis to the GI tract in 1965. The tumor was approximately of 6 cm, and located in the left hepatic lobe with portal vein invasion, and metastasized to the esophagus.2 Shiota et al. reported the first case of HCC with stomach invasion in which the tumor was located in both the right and left hepatic lobe.3
A systematic review published by Urhut et al. in 2022 included 192 patients, 87.3% of whom were male.1 According to the report, the most common GI tract metastases were in the stomach (27.9%) and duodenum (27.9%). Most routes of metastasis were direct invasion and hematogenous metastasis. Therefore, risk factors for HCC with GI tract metastases included growth mode, tumor size, tumor localization, and portal vein invasion. Because of their close anatomical location, tumors located on the right side of the liver are more likely to invade the duodenum, whereas tumors located on the left side of the liver are more likely to invade the stomach.1 Symptoms of HCC with GI invasion include GI bleeding, anemia, abdominal pain, palpable masses, nausea, and vomiting. Esophagogastroduodenoscopy and abdominal contrast-CT are the most useful diagnostic tools. Histological evidence can help diagnose HCC with GI invasion and differentiate between HCC and GI cancer. Immunohistochemical evidence for diagnosing HCC included Hep par-1, arginase-1, GPC-3, and polyclonal carcinoembryonic antigen.4 In addition, hepatoid adenocarcinoma, a rare extrahepatic adenocarcinoma, was a differential diagnosis of gastric tumor with high AFP.5
In conclusion, HCC with GI tract invasion as the first presentation is rare. However, HCC with GI metastasis should be considered when HCC patients present with GI bleeding and anemia. Endoscopy is the gold standard method for diagnosing HCC with GI tract invasion. Although many treatment strategies are available for HCC, the prognosis of patients with liver cancer complicated by GI metastases is poor.
The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


