{"title":"使用凹凸不平的双腔导管和支架回取器,通过肝胃造口术途径,在内窥镜下成功回取移位的胆道塑料支架。","authors":"Shingo Hirai, Yoshinobu Okabe, Shinichiro Yoshioka","doi":"10.1111/den.14868","DOIUrl":null,"url":null,"abstract":"<p>Our patient was an 80-year-old man with dementia and a history of distal gastrectomy and Roux-en-Y reconstruction after gastric cancer. He developed cholangitis due to common bile duct stones for which transpapillary endoscopic treatment using short single-balloon enteroscopy was unsuccessful. Managing percutaneous transhepatic biliary drainage was difficult; therefore, we chose endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS). A guidewire (0.025 inch GW) tip was advanced into the duodenum via the HGS route, and the straight-type plastic stent (PS) migrated during its antegrade placement. Another antegrade straight-type PS (7F, 10 cm) was placed across the papilla, and a tapered tip and 4-fold-flanged single-pigtail bile duct stent for EUS inferior drainage<span><sup>1</sup></span> (7F, 14 cm) were placed via the EUS-HGS route, and the cholangitis improved. At the family's request, the migrated PS was followed. Eleven months later, the patient developed acute cholangitis due to the PS obstruction. The obstructed stray PS causing cholangitis was to be retrieved by the HGS route (Video S1).<span><sup>2</sup></span> The GW was placed in the bile duct via the HGS route and the inside stent with thread was removed. Next, we attempted to retrieve the migrated PS using grasping and basket forceps via the same route; however, capturing the PS was extremely difficult (Fig. 1a). After the PS was moved to the papillary side using a balloon catheter, an uneven double-lumen catheter was placed in the bile duct via the HGS route and the GW was successfully inserted into the lumen of the migrated PS through the side hole of the catheter (Fig. 1b). Thereafter, we successfully recovered the PS using a Soehendra stent retriever (Cook Medical, Bloomington, IN) (Fig. 1c). Although it is often difficult to retrieve a migrated stent via the HGS route, the combined use of an uneven catheter and the Soehendra stent retriever<span><sup>3</sup></span> was successful in this case (Fig. 2).</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 8","pages":"959-960"},"PeriodicalIF":5.0000,"publicationDate":"2024-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14868","citationCount":"0","resultStr":"{\"title\":\"Successful endoscopic retrieval of migrated biliary plastic stent via hepaticogastrostomy route using uneven double-lumen catheter and stent retriever\",\"authors\":\"Shingo Hirai, Yoshinobu Okabe, Shinichiro Yoshioka\",\"doi\":\"10.1111/den.14868\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Our patient was an 80-year-old man with dementia and a history of distal gastrectomy and Roux-en-Y reconstruction after gastric cancer. He developed cholangitis due to common bile duct stones for which transpapillary endoscopic treatment using short single-balloon enteroscopy was unsuccessful. Managing percutaneous transhepatic biliary drainage was difficult; therefore, we chose endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS). A guidewire (0.025 inch GW) tip was advanced into the duodenum via the HGS route, and the straight-type plastic stent (PS) migrated during its antegrade placement. Another antegrade straight-type PS (7F, 10 cm) was placed across the papilla, and a tapered tip and 4-fold-flanged single-pigtail bile duct stent for EUS inferior drainage<span><sup>1</sup></span> (7F, 14 cm) were placed via the EUS-HGS route, and the cholangitis improved. At the family's request, the migrated PS was followed. Eleven months later, the patient developed acute cholangitis due to the PS obstruction. The obstructed stray PS causing cholangitis was to be retrieved by the HGS route (Video S1).<span><sup>2</sup></span> The GW was placed in the bile duct via the HGS route and the inside stent with thread was removed. Next, we attempted to retrieve the migrated PS using grasping and basket forceps via the same route; however, capturing the PS was extremely difficult (Fig. 1a). After the PS was moved to the papillary side using a balloon catheter, an uneven double-lumen catheter was placed in the bile duct via the HGS route and the GW was successfully inserted into the lumen of the migrated PS through the side hole of the catheter (Fig. 1b). Thereafter, we successfully recovered the PS using a Soehendra stent retriever (Cook Medical, Bloomington, IN) (Fig. 1c). Although it is often difficult to retrieve a migrated stent via the HGS route, the combined use of an uneven catheter and the Soehendra stent retriever<span><sup>3</sup></span> was successful in this case (Fig. 2).</p><p>Authors declare no conflict of interest for this article.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 8\",\"pages\":\"959-960\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14868\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14868\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14868","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Successful endoscopic retrieval of migrated biliary plastic stent via hepaticogastrostomy route using uneven double-lumen catheter and stent retriever
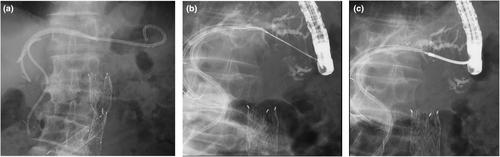
Our patient was an 80-year-old man with dementia and a history of distal gastrectomy and Roux-en-Y reconstruction after gastric cancer. He developed cholangitis due to common bile duct stones for which transpapillary endoscopic treatment using short single-balloon enteroscopy was unsuccessful. Managing percutaneous transhepatic biliary drainage was difficult; therefore, we chose endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS). A guidewire (0.025 inch GW) tip was advanced into the duodenum via the HGS route, and the straight-type plastic stent (PS) migrated during its antegrade placement. Another antegrade straight-type PS (7F, 10 cm) was placed across the papilla, and a tapered tip and 4-fold-flanged single-pigtail bile duct stent for EUS inferior drainage1 (7F, 14 cm) were placed via the EUS-HGS route, and the cholangitis improved. At the family's request, the migrated PS was followed. Eleven months later, the patient developed acute cholangitis due to the PS obstruction. The obstructed stray PS causing cholangitis was to be retrieved by the HGS route (Video S1).2 The GW was placed in the bile duct via the HGS route and the inside stent with thread was removed. Next, we attempted to retrieve the migrated PS using grasping and basket forceps via the same route; however, capturing the PS was extremely difficult (Fig. 1a). After the PS was moved to the papillary side using a balloon catheter, an uneven double-lumen catheter was placed in the bile duct via the HGS route and the GW was successfully inserted into the lumen of the migrated PS through the side hole of the catheter (Fig. 1b). Thereafter, we successfully recovered the PS using a Soehendra stent retriever (Cook Medical, Bloomington, IN) (Fig. 1c). Although it is often difficult to retrieve a migrated stent via the HGS route, the combined use of an uneven catheter and the Soehendra stent retriever3 was successful in this case (Fig. 2).
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


