{"title":"一名肠系膜绞窄疝患儿的延迟诊断。","authors":"Kenichi Tetsuhara, Kazunobu Nakabayashi, Mamoru Muraoka, Rie Kikuno, Michiko Ueda, Ryo Inoue, Makoto Hayashida","doi":"10.1002/ams2.977","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Strangulated intestinal obstruction is a life-threatening condition that should be considered as a differential diagnosis in children with shock. However, it has pitfalls in diagnosis and can lead to diagnostic errors.</p>\n </section>\n \n <section>\n \n <h3> Case Presentation</h3>\n \n <p>A 3-month-old male patient presented with a pale complexion lasting 2 h and abnormal crying. He was in shock with lactic acidosis, altered mental status, and slight abdominal distension. He required volume resuscitation, vasoactive agents, and transfusion. On Day 2, he had marked abdominal distension and acute kidney injury, which required continuous kidney replacement therapy. Contrast-enhanced computed tomography revealed extensive intestinal ischemia. It took 33.5 h from his arrival to the computed tomography, leading to operative management. The small intestine had entered a mesenteric hiatus, leading to ischemia. He was diagnosed with strangulated mesenteric hernia.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In this case, four pitfalls led to delayed diagnosis. Factors for diagnostic errors specific to strangulated intestinal obstruction and intensive care should be noted.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11184467/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed diagnosis in a child with strangulated mesenteric hernia\",\"authors\":\"Kenichi Tetsuhara, Kazunobu Nakabayashi, Mamoru Muraoka, Rie Kikuno, Michiko Ueda, Ryo Inoue, Makoto Hayashida\",\"doi\":\"10.1002/ams2.977\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Strangulated intestinal obstruction is a life-threatening condition that should be considered as a differential diagnosis in children with shock. However, it has pitfalls in diagnosis and can lead to diagnostic errors.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Case Presentation</h3>\\n \\n <p>A 3-month-old male patient presented with a pale complexion lasting 2 h and abnormal crying. He was in shock with lactic acidosis, altered mental status, and slight abdominal distension. He required volume resuscitation, vasoactive agents, and transfusion. On Day 2, he had marked abdominal distension and acute kidney injury, which required continuous kidney replacement therapy. Contrast-enhanced computed tomography revealed extensive intestinal ischemia. It took 33.5 h from his arrival to the computed tomography, leading to operative management. The small intestine had entered a mesenteric hiatus, leading to ischemia. He was diagnosed with strangulated mesenteric hernia.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In this case, four pitfalls led to delayed diagnosis. Factors for diagnostic errors specific to strangulated intestinal obstruction and intensive care should be noted.</p>\\n </section>\\n </div>\",\"PeriodicalId\":7196,\"journal\":{\"name\":\"Acute Medicine & Surgery\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11184467/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute Medicine & Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ams2.977\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.977","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Delayed diagnosis in a child with strangulated mesenteric hernia
Background
Strangulated intestinal obstruction is a life-threatening condition that should be considered as a differential diagnosis in children with shock. However, it has pitfalls in diagnosis and can lead to diagnostic errors.
Case Presentation
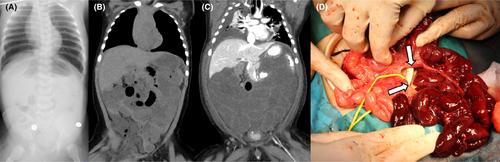
A 3-month-old male patient presented with a pale complexion lasting 2 h and abnormal crying. He was in shock with lactic acidosis, altered mental status, and slight abdominal distension. He required volume resuscitation, vasoactive agents, and transfusion. On Day 2, he had marked abdominal distension and acute kidney injury, which required continuous kidney replacement therapy. Contrast-enhanced computed tomography revealed extensive intestinal ischemia. It took 33.5 h from his arrival to the computed tomography, leading to operative management. The small intestine had entered a mesenteric hiatus, leading to ischemia. He was diagnosed with strangulated mesenteric hernia.
Conclusion
In this case, four pitfalls led to delayed diagnosis. Factors for diagnostic errors specific to strangulated intestinal obstruction and intensive care should be noted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


