{"title":"WEO 简讯:内镜下有效闭合胃肠道缺损的策略","authors":"","doi":"10.1111/den.14858","DOIUrl":null,"url":null,"abstract":"<p>Gaurav Kakked MD and Christopher G. Chapman MD</p><p>Endoscopic techniques have advanced significantly, offering new avenues for treating gastrointestinal defects ranging from full-thickness perforations to more superficial lesions. Effective management of these defects is crucial to prevent complications and improve patient outcomes. This article provides a guide on the strategies and considerations necessary for successful endoscopic closure of gastrointestinal defects.</p><p>The first step in managing gastrointestinal defects is to clearly define the type of defect being treated:</p><p>• Full-thickness defects, such as acute perforations, postoperative leaks, and fistulas, involve all layers of the gastrointestinal wall (Figure 1A–C). Full-thickness defects are “higher stakes” as they permit spillage of gastrointestinal contents into the sterile abdominal cavity, leading to peritonitis, abscesses, and potential septic complications. Full-thickness defects tend to be complex and their closure requires a multidisciplinary approach including nutritional support, infection control and, potentially, surgical, endoscopic, or radiological intervention.</p><p>• Non-full-thickness defects include endoscopic resection defects and submucosal incisions. These tend to be “lower stakes” as they remain sterile, but successful closure is important to prevent delayed complications such as perforation or bleeding.</p><p>Differentiating between these two types of defect is crucial as it dictates the risk/benefit profile, approach, tools, and techniques used during the closure process.</p><p>The anatomical location and size of the defect significantly affects the approach and can determine what devices will be appropriate for use. If a defect is in a hard-to-reach area, such as the proximal esophagus, gastric fundus, duodenum/jejunum, or right colon, then through-the-scope (TTS) approaches might be the only available option. Recent advances have introduced TTS suture-based devices that allow for deep submucosal and intramuscular fixation, expanding the possibilities for effective closure even in difficult-to-reach areas.</p><p>If a defect is smaller in size, even if it is full thickness such as an acute perforation, then TTS or over-the-scope (OTS) clipping may be sufficient. While closure of larger-size defects (>2–3 cm) can be attempted with multiple TTS clips, we are quick to consider endoscopic suturing (TTS or OTS) and/or stent placement.</p><p>Another point to bear in mind is that acute perforation can be one of the full-thickness defects most amenable to closure because of the presence of healthy tissue at the margin of the defect. Thus, the “clock is ticking” after an acute perforation and emergent endoscopy is necessary to attempt closure while the adjacent tissue is still healthy. However, leaks and fistulas tend to be complex with unhealthy (fibrotic or inflamed) tissue; thus direct endoscopic closure techniques are often ineffective, and transition to coverage techniques (stenting) or innovative methods (endoscopic vacuum therapy [EVT]) is required.</p><p>Embarking on the successful closure of gastrointestinal defects involves several critical steps to ensure safety, technical success, and clinical efficacy. Consider implementing a preprocedural checklist for defect closure:</p><p>(i) Assess patient stability: Prior to preforming endoscopy, patient hemodynamic stability must be assessed to determine whether endoscopy is appropriate; in cases where the patient is unstable, early surgical intervention might be necessary.</p><p>(ii) Review or obtain cross-sectional imaging: Cross-sectional or fluoroscopic imaging with water-soluble contrast is essential to accurately evaluate the extent and location of full-thickness defects.</p><p>(iii) Ensure the “in-room” availability of essential equipment: The therapeutic toolbox for defect closure is extensive and not always immediately available when time is of the essence. Try to predict what tools will be needed and have them obtained prior to the procedure.</p><p>(iv) Appropriate anesthesia selection/communication: Frequently, general anesthesia will be required to minimize the risk of procedural complication.</p><p>(v) Obtain appropriate surgical or interventional radiology back-up.</p><p>(vi) Use of CO2 for insufflation.</p><p>(vii) Obtain informed consent. Often with full-thickness defects, you will be working to salvage a complication or you might end up using equipment for off-label purposes; we recommend discussing with the patient and family the risks, benefits, and plans prior to the procedure.</p><p>(viii) Obtain a fluoroscopy “scout film” prior to starting your procedure. A prior scout film will allow for a reference comparison as the procedure continues and interventions are performed.</p><p>These preparatory measures are foundational in creating a controlled and secure environment for conducting closure of a gastrointestinal defect.</p><p>Full-thickness defects are frequently associated with leakage of gastrointestinal contents into sterile spaces, which can form collections adjacent to the area of the defect. Undrained fluid collections can lead to worsening infection and prevent definitive closure of full-thickness defects. Drainage should be pursued through surgical, radiologic/percutaneous, or endoscopic approaches. Given that drainage should be completed simultaneously with attempted defect closure or covering, we recommend reviewing cross-sectional imaging with the surgery/interventional radiology teams prior to endoscopy to help with planning. In certain situations, such as proximal gastric sleeve leaks, radiology may not provide a safe window for percutaneous drainage, and endoscopic drainage with plastic pigtail stents may be the only option (Figure 2A–F).</p><p>Reducing downstream obstructions in the gastrointestinal tract is crucial for decreasing back pressure on defects, thereby enhancing the chances of successful closure. One effective technique is balloon dilation, which utilizes either pneumatic or hydrostatic balloons to dilate narrowed areas downstream from the defect. This method is particularly valuable in post-bariatric/surgical stenoses, as it improves flow dynamics and facilitates the resolution of fistulas and leaks. Additionally, managing other downstream medical conditions, such as an ileus or even constipation, can also alleviate back pressure on the defect site and further aid in the healing process.</p><p>Fully covered self-expandable metal stents (FCSEMSs) can effectively cover full-thickness defects and allow for healing; however, clinical success requires not only precise placement, but also maintenance of the location. The coating of FCSEMSs makes them valuable for their ease of removal due to lack of tissue ingrowth, but renders them prone to distal migration and therefore reduced clinical success. To decrease the risk of migration, we recommend endoscopic stent fixation, of which there are two acceptable methods: endoscopic suturing (Figure 3A,B) and OTS clipping (Figure 3C,D).</p><p>If performing endoscopic suturing for stent fixation, we recommend the following:</p><p>(i) Use at least two sutures if possible: Plan to use multiple points of fixation as this will decrease the likelihood of distal migration.</p><p>(ii) Do not use the tissue helix to grasp tissue: Full-thickness bites are not required and the use of the tissue helix in the esophagus can lead to unintentional injury to adjacent structures. Often, just applying suction with the scope will allow for satisfactory tissue acquisition for stent fixation.</p><p>(iii) Be precise with your suture placement: Under direct visualization, aim to pass the suture through at least 2–3 interstices while avoiding the metal structure and removal suture. If the stent does not easily come into the path of the needle body, use a biopsy forceps to grasp the stent and bring it to the optimal position.</p><p>(iv) Do not overtighten the cinch: Overtightening the cinch will make it increasingly difficult to cut the suture with a loop cutter, argon plasma coagulation (APC), or endoscopic scissors prior to removal.</p><p>Alternatively, an OTS clip designed for stent fixation offers mechanical fixation by clamping onto both the stent and the gastrointestinal wall, thus ensuring a firm hold. However, standard removal techniques require the purchase and use of a separate generator and probe technology.</p><p>Chronic fistula tracts often become resistant to endoscopic treatment because of epithelialization and fibrosis. In attempting endoscopic treatment of chronic fistulas, manage patient expectations appropriately, being clear that endoscopy often fails and repeated attempts at closure may be necessary. Various endoscopic techniques, such as clipping, stenting, endoscopic suturing, and tissue sealing with for example fibrin glue can be employed, based on fistula characteristics including size and location. However, epithelialization hinders the healing process. This must be addressed by removal of foreign body material (surgical clips/sutures), and tissue debridement using APC or a cytology brush, or by endoscopic submucosal dissection, to facilitate healing.</p><p>Needle decompression for tension pneumoperitoneum may be a potentially lifesaving intervention for an unstable endoscopic patient with a full-thickness defect. When performing endoscopic procedures with risk of perforation, we recommend having a large-gauge needle, such as a Veress needle or a 14- to 16-gauge angiocath needle, to relieve pressure and prevent further complications. We recommend listening to cues from your anesthesia team, including unexpected “high peak pressures,” “difficulty ventilating” or “low tidal volumes.” Any of these prompts should lead you to feel the abdomen and consider emergent decompression if the abdomen is firm and distended.</p><p>Nutrition plays a vital role in the process of recovery from gastrointestinal defects. Enteral feeding is generally preferred over parenteral nutrition because of its ability to utilize the gut, which helps maintain the integrity of the intestinal mucosa and reduces infection risks. After defect closure, ensure that there is a plan for effective nutritional support. This could include placement of a nasojejunal tube (NJT) for short-term needs, or a percutaneous endoscopic gastrostomy (PEG) or jejunostomy (PEJ) tube for patients requiring long-term nutritional support. Total parenteral nutrition (TPN) should be avoided if possible.</p><p>The task is not done when defect closure is completed. Post-procedure monitoring is essential to assess the success of the closure. When using metal stents, we recommend obtaining serial imaging to check stent position and apposition. This is important, bearing in mind that fully covered metal stents can migrate and foreshorten, requiring adjustments or additional interventions. Additionally, ensure that all implantable devices are removed as scheduled to prevent device-related complications.</p><p>We recommend staying open to using novel techniques such as EVT, septotomy, percutaneous suturing, and the use of non-gastroenterological devices (e.g. cardiac septal occluder), which can offer alternative solutions, particularly in cases of complex refractory defects.</p><p>The endoscopic closure of gastrointestinal defects requires a detailed understanding of defect type, location, and appropriate management strategies. By integrating advanced techniques and thorough preparation, clinicians can effectively manage these challenging conditions, improving patient outcomes and reducing complications.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 6","pages":"751-755"},"PeriodicalIF":5.0000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14858","citationCount":"0","resultStr":"{\"title\":\"WEO Newsletter: Strategies for effective endoscopic closure of gastrointestinal defects\",\"authors\":\"\",\"doi\":\"10.1111/den.14858\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Gaurav Kakked MD and Christopher G. Chapman MD</p><p>Endoscopic techniques have advanced significantly, offering new avenues for treating gastrointestinal defects ranging from full-thickness perforations to more superficial lesions. Effective management of these defects is crucial to prevent complications and improve patient outcomes. This article provides a guide on the strategies and considerations necessary for successful endoscopic closure of gastrointestinal defects.</p><p>The first step in managing gastrointestinal defects is to clearly define the type of defect being treated:</p><p>• Full-thickness defects, such as acute perforations, postoperative leaks, and fistulas, involve all layers of the gastrointestinal wall (Figure 1A–C). Full-thickness defects are “higher stakes” as they permit spillage of gastrointestinal contents into the sterile abdominal cavity, leading to peritonitis, abscesses, and potential septic complications. Full-thickness defects tend to be complex and their closure requires a multidisciplinary approach including nutritional support, infection control and, potentially, surgical, endoscopic, or radiological intervention.</p><p>• Non-full-thickness defects include endoscopic resection defects and submucosal incisions. These tend to be “lower stakes” as they remain sterile, but successful closure is important to prevent delayed complications such as perforation or bleeding.</p><p>Differentiating between these two types of defect is crucial as it dictates the risk/benefit profile, approach, tools, and techniques used during the closure process.</p><p>The anatomical location and size of the defect significantly affects the approach and can determine what devices will be appropriate for use. If a defect is in a hard-to-reach area, such as the proximal esophagus, gastric fundus, duodenum/jejunum, or right colon, then through-the-scope (TTS) approaches might be the only available option. Recent advances have introduced TTS suture-based devices that allow for deep submucosal and intramuscular fixation, expanding the possibilities for effective closure even in difficult-to-reach areas.</p><p>If a defect is smaller in size, even if it is full thickness such as an acute perforation, then TTS or over-the-scope (OTS) clipping may be sufficient. While closure of larger-size defects (>2–3 cm) can be attempted with multiple TTS clips, we are quick to consider endoscopic suturing (TTS or OTS) and/or stent placement.</p><p>Another point to bear in mind is that acute perforation can be one of the full-thickness defects most amenable to closure because of the presence of healthy tissue at the margin of the defect. Thus, the “clock is ticking” after an acute perforation and emergent endoscopy is necessary to attempt closure while the adjacent tissue is still healthy. However, leaks and fistulas tend to be complex with unhealthy (fibrotic or inflamed) tissue; thus direct endoscopic closure techniques are often ineffective, and transition to coverage techniques (stenting) or innovative methods (endoscopic vacuum therapy [EVT]) is required.</p><p>Embarking on the successful closure of gastrointestinal defects involves several critical steps to ensure safety, technical success, and clinical efficacy. Consider implementing a preprocedural checklist for defect closure:</p><p>(i) Assess patient stability: Prior to preforming endoscopy, patient hemodynamic stability must be assessed to determine whether endoscopy is appropriate; in cases where the patient is unstable, early surgical intervention might be necessary.</p><p>(ii) Review or obtain cross-sectional imaging: Cross-sectional or fluoroscopic imaging with water-soluble contrast is essential to accurately evaluate the extent and location of full-thickness defects.</p><p>(iii) Ensure the “in-room” availability of essential equipment: The therapeutic toolbox for defect closure is extensive and not always immediately available when time is of the essence. Try to predict what tools will be needed and have them obtained prior to the procedure.</p><p>(iv) Appropriate anesthesia selection/communication: Frequently, general anesthesia will be required to minimize the risk of procedural complication.</p><p>(v) Obtain appropriate surgical or interventional radiology back-up.</p><p>(vi) Use of CO2 for insufflation.</p><p>(vii) Obtain informed consent. Often with full-thickness defects, you will be working to salvage a complication or you might end up using equipment for off-label purposes; we recommend discussing with the patient and family the risks, benefits, and plans prior to the procedure.</p><p>(viii) Obtain a fluoroscopy “scout film” prior to starting your procedure. A prior scout film will allow for a reference comparison as the procedure continues and interventions are performed.</p><p>These preparatory measures are foundational in creating a controlled and secure environment for conducting closure of a gastrointestinal defect.</p><p>Full-thickness defects are frequently associated with leakage of gastrointestinal contents into sterile spaces, which can form collections adjacent to the area of the defect. Undrained fluid collections can lead to worsening infection and prevent definitive closure of full-thickness defects. Drainage should be pursued through surgical, radiologic/percutaneous, or endoscopic approaches. Given that drainage should be completed simultaneously with attempted defect closure or covering, we recommend reviewing cross-sectional imaging with the surgery/interventional radiology teams prior to endoscopy to help with planning. In certain situations, such as proximal gastric sleeve leaks, radiology may not provide a safe window for percutaneous drainage, and endoscopic drainage with plastic pigtail stents may be the only option (Figure 2A–F).</p><p>Reducing downstream obstructions in the gastrointestinal tract is crucial for decreasing back pressure on defects, thereby enhancing the chances of successful closure. One effective technique is balloon dilation, which utilizes either pneumatic or hydrostatic balloons to dilate narrowed areas downstream from the defect. This method is particularly valuable in post-bariatric/surgical stenoses, as it improves flow dynamics and facilitates the resolution of fistulas and leaks. Additionally, managing other downstream medical conditions, such as an ileus or even constipation, can also alleviate back pressure on the defect site and further aid in the healing process.</p><p>Fully covered self-expandable metal stents (FCSEMSs) can effectively cover full-thickness defects and allow for healing; however, clinical success requires not only precise placement, but also maintenance of the location. The coating of FCSEMSs makes them valuable for their ease of removal due to lack of tissue ingrowth, but renders them prone to distal migration and therefore reduced clinical success. To decrease the risk of migration, we recommend endoscopic stent fixation, of which there are two acceptable methods: endoscopic suturing (Figure 3A,B) and OTS clipping (Figure 3C,D).</p><p>If performing endoscopic suturing for stent fixation, we recommend the following:</p><p>(i) Use at least two sutures if possible: Plan to use multiple points of fixation as this will decrease the likelihood of distal migration.</p><p>(ii) Do not use the tissue helix to grasp tissue: Full-thickness bites are not required and the use of the tissue helix in the esophagus can lead to unintentional injury to adjacent structures. Often, just applying suction with the scope will allow for satisfactory tissue acquisition for stent fixation.</p><p>(iii) Be precise with your suture placement: Under direct visualization, aim to pass the suture through at least 2–3 interstices while avoiding the metal structure and removal suture. If the stent does not easily come into the path of the needle body, use a biopsy forceps to grasp the stent and bring it to the optimal position.</p><p>(iv) Do not overtighten the cinch: Overtightening the cinch will make it increasingly difficult to cut the suture with a loop cutter, argon plasma coagulation (APC), or endoscopic scissors prior to removal.</p><p>Alternatively, an OTS clip designed for stent fixation offers mechanical fixation by clamping onto both the stent and the gastrointestinal wall, thus ensuring a firm hold. However, standard removal techniques require the purchase and use of a separate generator and probe technology.</p><p>Chronic fistula tracts often become resistant to endoscopic treatment because of epithelialization and fibrosis. In attempting endoscopic treatment of chronic fistulas, manage patient expectations appropriately, being clear that endoscopy often fails and repeated attempts at closure may be necessary. Various endoscopic techniques, such as clipping, stenting, endoscopic suturing, and tissue sealing with for example fibrin glue can be employed, based on fistula characteristics including size and location. However, epithelialization hinders the healing process. This must be addressed by removal of foreign body material (surgical clips/sutures), and tissue debridement using APC or a cytology brush, or by endoscopic submucosal dissection, to facilitate healing.</p><p>Needle decompression for tension pneumoperitoneum may be a potentially lifesaving intervention for an unstable endoscopic patient with a full-thickness defect. When performing endoscopic procedures with risk of perforation, we recommend having a large-gauge needle, such as a Veress needle or a 14- to 16-gauge angiocath needle, to relieve pressure and prevent further complications. We recommend listening to cues from your anesthesia team, including unexpected “high peak pressures,” “difficulty ventilating” or “low tidal volumes.” Any of these prompts should lead you to feel the abdomen and consider emergent decompression if the abdomen is firm and distended.</p><p>Nutrition plays a vital role in the process of recovery from gastrointestinal defects. Enteral feeding is generally preferred over parenteral nutrition because of its ability to utilize the gut, which helps maintain the integrity of the intestinal mucosa and reduces infection risks. After defect closure, ensure that there is a plan for effective nutritional support. This could include placement of a nasojejunal tube (NJT) for short-term needs, or a percutaneous endoscopic gastrostomy (PEG) or jejunostomy (PEJ) tube for patients requiring long-term nutritional support. Total parenteral nutrition (TPN) should be avoided if possible.</p><p>The task is not done when defect closure is completed. Post-procedure monitoring is essential to assess the success of the closure. When using metal stents, we recommend obtaining serial imaging to check stent position and apposition. This is important, bearing in mind that fully covered metal stents can migrate and foreshorten, requiring adjustments or additional interventions. Additionally, ensure that all implantable devices are removed as scheduled to prevent device-related complications.</p><p>We recommend staying open to using novel techniques such as EVT, septotomy, percutaneous suturing, and the use of non-gastroenterological devices (e.g. cardiac septal occluder), which can offer alternative solutions, particularly in cases of complex refractory defects.</p><p>The endoscopic closure of gastrointestinal defects requires a detailed understanding of defect type, location, and appropriate management strategies. By integrating advanced techniques and thorough preparation, clinicians can effectively manage these challenging conditions, improving patient outcomes and reducing complications.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 6\",\"pages\":\"751-755\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14858\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14858\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14858","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
WEO Newsletter: Strategies for effective endoscopic closure of gastrointestinal defects
Gaurav Kakked MD and Christopher G. Chapman MD
Endoscopic techniques have advanced significantly, offering new avenues for treating gastrointestinal defects ranging from full-thickness perforations to more superficial lesions. Effective management of these defects is crucial to prevent complications and improve patient outcomes. This article provides a guide on the strategies and considerations necessary for successful endoscopic closure of gastrointestinal defects.
The first step in managing gastrointestinal defects is to clearly define the type of defect being treated:
• Full-thickness defects, such as acute perforations, postoperative leaks, and fistulas, involve all layers of the gastrointestinal wall (Figure 1A–C). Full-thickness defects are “higher stakes” as they permit spillage of gastrointestinal contents into the sterile abdominal cavity, leading to peritonitis, abscesses, and potential septic complications. Full-thickness defects tend to be complex and their closure requires a multidisciplinary approach including nutritional support, infection control and, potentially, surgical, endoscopic, or radiological intervention.
• Non-full-thickness defects include endoscopic resection defects and submucosal incisions. These tend to be “lower stakes” as they remain sterile, but successful closure is important to prevent delayed complications such as perforation or bleeding.
Differentiating between these two types of defect is crucial as it dictates the risk/benefit profile, approach, tools, and techniques used during the closure process.
The anatomical location and size of the defect significantly affects the approach and can determine what devices will be appropriate for use. If a defect is in a hard-to-reach area, such as the proximal esophagus, gastric fundus, duodenum/jejunum, or right colon, then through-the-scope (TTS) approaches might be the only available option. Recent advances have introduced TTS suture-based devices that allow for deep submucosal and intramuscular fixation, expanding the possibilities for effective closure even in difficult-to-reach areas.
If a defect is smaller in size, even if it is full thickness such as an acute perforation, then TTS or over-the-scope (OTS) clipping may be sufficient. While closure of larger-size defects (>2–3 cm) can be attempted with multiple TTS clips, we are quick to consider endoscopic suturing (TTS or OTS) and/or stent placement.
Another point to bear in mind is that acute perforation can be one of the full-thickness defects most amenable to closure because of the presence of healthy tissue at the margin of the defect. Thus, the “clock is ticking” after an acute perforation and emergent endoscopy is necessary to attempt closure while the adjacent tissue is still healthy. However, leaks and fistulas tend to be complex with unhealthy (fibrotic or inflamed) tissue; thus direct endoscopic closure techniques are often ineffective, and transition to coverage techniques (stenting) or innovative methods (endoscopic vacuum therapy [EVT]) is required.
Embarking on the successful closure of gastrointestinal defects involves several critical steps to ensure safety, technical success, and clinical efficacy. Consider implementing a preprocedural checklist for defect closure:
(i) Assess patient stability: Prior to preforming endoscopy, patient hemodynamic stability must be assessed to determine whether endoscopy is appropriate; in cases where the patient is unstable, early surgical intervention might be necessary.
(ii) Review or obtain cross-sectional imaging: Cross-sectional or fluoroscopic imaging with water-soluble contrast is essential to accurately evaluate the extent and location of full-thickness defects.
(iii) Ensure the “in-room” availability of essential equipment: The therapeutic toolbox for defect closure is extensive and not always immediately available when time is of the essence. Try to predict what tools will be needed and have them obtained prior to the procedure.
(iv) Appropriate anesthesia selection/communication: Frequently, general anesthesia will be required to minimize the risk of procedural complication.
(v) Obtain appropriate surgical or interventional radiology back-up.
(vi) Use of CO2 for insufflation.
(vii) Obtain informed consent. Often with full-thickness defects, you will be working to salvage a complication or you might end up using equipment for off-label purposes; we recommend discussing with the patient and family the risks, benefits, and plans prior to the procedure.
(viii) Obtain a fluoroscopy “scout film” prior to starting your procedure. A prior scout film will allow for a reference comparison as the procedure continues and interventions are performed.
These preparatory measures are foundational in creating a controlled and secure environment for conducting closure of a gastrointestinal defect.
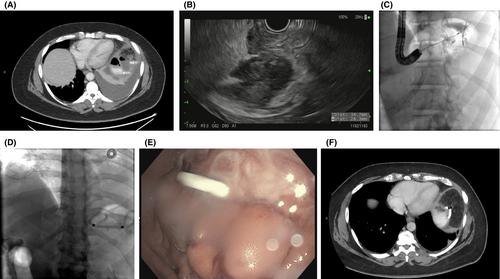
Full-thickness defects are frequently associated with leakage of gastrointestinal contents into sterile spaces, which can form collections adjacent to the area of the defect. Undrained fluid collections can lead to worsening infection and prevent definitive closure of full-thickness defects. Drainage should be pursued through surgical, radiologic/percutaneous, or endoscopic approaches. Given that drainage should be completed simultaneously with attempted defect closure or covering, we recommend reviewing cross-sectional imaging with the surgery/interventional radiology teams prior to endoscopy to help with planning. In certain situations, such as proximal gastric sleeve leaks, radiology may not provide a safe window for percutaneous drainage, and endoscopic drainage with plastic pigtail stents may be the only option (Figure 2A–F).
Reducing downstream obstructions in the gastrointestinal tract is crucial for decreasing back pressure on defects, thereby enhancing the chances of successful closure. One effective technique is balloon dilation, which utilizes either pneumatic or hydrostatic balloons to dilate narrowed areas downstream from the defect. This method is particularly valuable in post-bariatric/surgical stenoses, as it improves flow dynamics and facilitates the resolution of fistulas and leaks. Additionally, managing other downstream medical conditions, such as an ileus or even constipation, can also alleviate back pressure on the defect site and further aid in the healing process.
Fully covered self-expandable metal stents (FCSEMSs) can effectively cover full-thickness defects and allow for healing; however, clinical success requires not only precise placement, but also maintenance of the location. The coating of FCSEMSs makes them valuable for their ease of removal due to lack of tissue ingrowth, but renders them prone to distal migration and therefore reduced clinical success. To decrease the risk of migration, we recommend endoscopic stent fixation, of which there are two acceptable methods: endoscopic suturing (Figure 3A,B) and OTS clipping (Figure 3C,D).
If performing endoscopic suturing for stent fixation, we recommend the following:
(i) Use at least two sutures if possible: Plan to use multiple points of fixation as this will decrease the likelihood of distal migration.
(ii) Do not use the tissue helix to grasp tissue: Full-thickness bites are not required and the use of the tissue helix in the esophagus can lead to unintentional injury to adjacent structures. Often, just applying suction with the scope will allow for satisfactory tissue acquisition for stent fixation.
(iii) Be precise with your suture placement: Under direct visualization, aim to pass the suture through at least 2–3 interstices while avoiding the metal structure and removal suture. If the stent does not easily come into the path of the needle body, use a biopsy forceps to grasp the stent and bring it to the optimal position.
(iv) Do not overtighten the cinch: Overtightening the cinch will make it increasingly difficult to cut the suture with a loop cutter, argon plasma coagulation (APC), or endoscopic scissors prior to removal.
Alternatively, an OTS clip designed for stent fixation offers mechanical fixation by clamping onto both the stent and the gastrointestinal wall, thus ensuring a firm hold. However, standard removal techniques require the purchase and use of a separate generator and probe technology.
Chronic fistula tracts often become resistant to endoscopic treatment because of epithelialization and fibrosis. In attempting endoscopic treatment of chronic fistulas, manage patient expectations appropriately, being clear that endoscopy often fails and repeated attempts at closure may be necessary. Various endoscopic techniques, such as clipping, stenting, endoscopic suturing, and tissue sealing with for example fibrin glue can be employed, based on fistula characteristics including size and location. However, epithelialization hinders the healing process. This must be addressed by removal of foreign body material (surgical clips/sutures), and tissue debridement using APC or a cytology brush, or by endoscopic submucosal dissection, to facilitate healing.
Needle decompression for tension pneumoperitoneum may be a potentially lifesaving intervention for an unstable endoscopic patient with a full-thickness defect. When performing endoscopic procedures with risk of perforation, we recommend having a large-gauge needle, such as a Veress needle or a 14- to 16-gauge angiocath needle, to relieve pressure and prevent further complications. We recommend listening to cues from your anesthesia team, including unexpected “high peak pressures,” “difficulty ventilating” or “low tidal volumes.” Any of these prompts should lead you to feel the abdomen and consider emergent decompression if the abdomen is firm and distended.
Nutrition plays a vital role in the process of recovery from gastrointestinal defects. Enteral feeding is generally preferred over parenteral nutrition because of its ability to utilize the gut, which helps maintain the integrity of the intestinal mucosa and reduces infection risks. After defect closure, ensure that there is a plan for effective nutritional support. This could include placement of a nasojejunal tube (NJT) for short-term needs, or a percutaneous endoscopic gastrostomy (PEG) or jejunostomy (PEJ) tube for patients requiring long-term nutritional support. Total parenteral nutrition (TPN) should be avoided if possible.
The task is not done when defect closure is completed. Post-procedure monitoring is essential to assess the success of the closure. When using metal stents, we recommend obtaining serial imaging to check stent position and apposition. This is important, bearing in mind that fully covered metal stents can migrate and foreshorten, requiring adjustments or additional interventions. Additionally, ensure that all implantable devices are removed as scheduled to prevent device-related complications.
We recommend staying open to using novel techniques such as EVT, septotomy, percutaneous suturing, and the use of non-gastroenterological devices (e.g. cardiac septal occluder), which can offer alternative solutions, particularly in cases of complex refractory defects.
The endoscopic closure of gastrointestinal defects requires a detailed understanding of defect type, location, and appropriate management strategies. By integrating advanced techniques and thorough preparation, clinicians can effectively manage these challenging conditions, improving patient outcomes and reducing complications.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


