Nicholas Beam, Allison Long, Adam Nicholson, Lauren Jary, Rebecca Veele, Nicole Kalinowski, Matthew Phad, Andrea Hadley
{"title":"优先考虑支气管炎肠内喂养的质量倡议。","authors":"Nicholas Beam, Allison Long, Adam Nicholson, Lauren Jary, Rebecca Veele, Nicole Kalinowski, Matthew Phad, Andrea Hadley","doi":"10.1097/pq9.0000000000000735","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Recent studies have identified enteral feeding as a safe alternative to intravenous fluid hydration for inpatients with bronchiolitis receiving respiratory support. Specifically, it can improve vital signs, shorten time on high-flow nasal cannula, and is associated with reduced length of stay. We aimed to increase the percentage of patients receiving enteral feeding on admission with mild-to-moderate bronchiolitis, including those on high-flow nasal cannula, from 83% to 95% within 6 months.</p><p><strong>Methods: </strong>A multidisciplinary quality improvement team identified key drivers preventing enteral feeding as lack of standardization, perception of aspiration risk, and lack of familiarity with feeding orders. PDSA cycles focused on developing and implementing a bronchiolitis clinical practice pathway with an embedded guideline and order set as decision support to prioritize enteral feeding. Additionally, educational sessions were provided for trainees and attendings who were impacted by this pathway.</p><p><strong>Results: </strong>Following interventions, initiation of enteral feeding increased (83%-96%). Additionally, intravenous line placement decreased (37%-12%) with a mirrored increase in nasogastric tube placement (4%-21%). This was associated with a shorter overall length of stay and no increased transfer rate to intensive care.</p><p><strong>Conclusions: </strong>Using quality improvement methodology to standardize enteral feeding and hydration increased the initiation rate of enteral feeding in patients admitted with bronchiolitis. These changes were seen immediately after the implementation of the clinical pathway and sustained throughout the bronchiolitis season.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e735"},"PeriodicalIF":1.1000,"publicationDate":"2024-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11167230/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Quality Initiative to Prioritize Enteral Feeding in Bronchiolitis.\",\"authors\":\"Nicholas Beam, Allison Long, Adam Nicholson, Lauren Jary, Rebecca Veele, Nicole Kalinowski, Matthew Phad, Andrea Hadley\",\"doi\":\"10.1097/pq9.0000000000000735\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Recent studies have identified enteral feeding as a safe alternative to intravenous fluid hydration for inpatients with bronchiolitis receiving respiratory support. Specifically, it can improve vital signs, shorten time on high-flow nasal cannula, and is associated with reduced length of stay. We aimed to increase the percentage of patients receiving enteral feeding on admission with mild-to-moderate bronchiolitis, including those on high-flow nasal cannula, from 83% to 95% within 6 months.</p><p><strong>Methods: </strong>A multidisciplinary quality improvement team identified key drivers preventing enteral feeding as lack of standardization, perception of aspiration risk, and lack of familiarity with feeding orders. PDSA cycles focused on developing and implementing a bronchiolitis clinical practice pathway with an embedded guideline and order set as decision support to prioritize enteral feeding. Additionally, educational sessions were provided for trainees and attendings who were impacted by this pathway.</p><p><strong>Results: </strong>Following interventions, initiation of enteral feeding increased (83%-96%). Additionally, intravenous line placement decreased (37%-12%) with a mirrored increase in nasogastric tube placement (4%-21%). This was associated with a shorter overall length of stay and no increased transfer rate to intensive care.</p><p><strong>Conclusions: </strong>Using quality improvement methodology to standardize enteral feeding and hydration increased the initiation rate of enteral feeding in patients admitted with bronchiolitis. These changes were seen immediately after the implementation of the clinical pathway and sustained throughout the bronchiolitis season.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 3\",\"pages\":\"e735\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-06-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11167230/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000735\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000735","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
A Quality Initiative to Prioritize Enteral Feeding in Bronchiolitis.
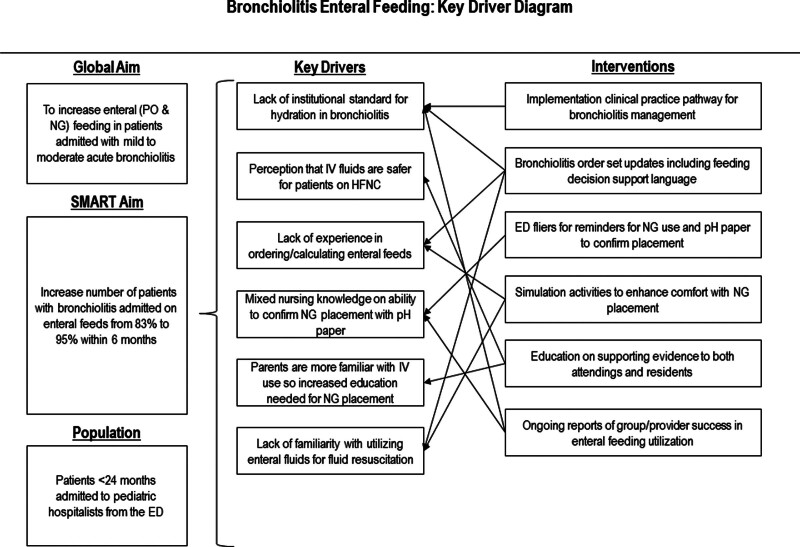
Introduction: Recent studies have identified enteral feeding as a safe alternative to intravenous fluid hydration for inpatients with bronchiolitis receiving respiratory support. Specifically, it can improve vital signs, shorten time on high-flow nasal cannula, and is associated with reduced length of stay. We aimed to increase the percentage of patients receiving enteral feeding on admission with mild-to-moderate bronchiolitis, including those on high-flow nasal cannula, from 83% to 95% within 6 months.
Methods: A multidisciplinary quality improvement team identified key drivers preventing enteral feeding as lack of standardization, perception of aspiration risk, and lack of familiarity with feeding orders. PDSA cycles focused on developing and implementing a bronchiolitis clinical practice pathway with an embedded guideline and order set as decision support to prioritize enteral feeding. Additionally, educational sessions were provided for trainees and attendings who were impacted by this pathway.
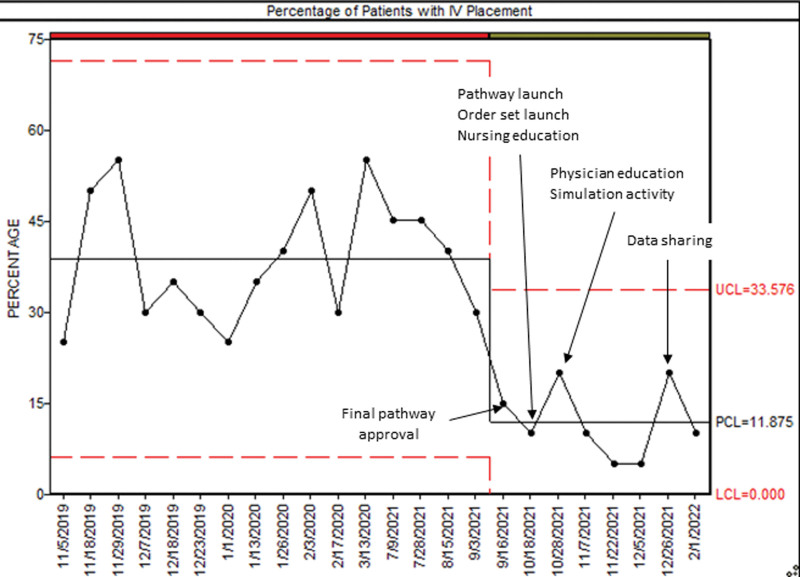
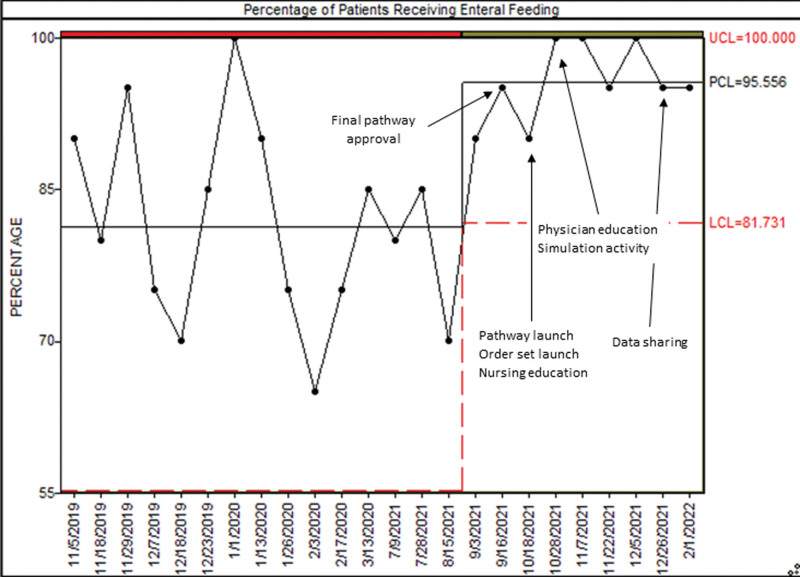
Results: Following interventions, initiation of enteral feeding increased (83%-96%). Additionally, intravenous line placement decreased (37%-12%) with a mirrored increase in nasogastric tube placement (4%-21%). This was associated with a shorter overall length of stay and no increased transfer rate to intensive care.
Conclusions: Using quality improvement methodology to standardize enteral feeding and hydration increased the initiation rate of enteral feeding in patients admitted with bronchiolitis. These changes were seen immediately after the implementation of the clinical pathway and sustained throughout the bronchiolitis season.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


