{"title":"哮喘患者小气道功能指标与呼吸道症状和合并症的关系:全国横断面研究","authors":"Jia Wei Long, Yong Liang Jiang","doi":"10.14740/jocmr5158","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Small airway dysfunction (SAD) and airway inflammation are vital in asthma exacerbations. Type 2 inflammation (T2), mediated by cytokines from T helper 2 cell (Th2) such as interleukin (IL)-4, IL-5, and IL-13, is a potential mechanism underlying SAD. Research on small airway function in asthma is limited. We aimed to explore the correlation between small airway function and respiratory symptoms and comorbidity in T2 and non-T2 asthma.</p><p><strong>Methods: </strong>Derived from the National Health and Nutrition Examination Survey (NHANES), our study encompassed 2,420 asthma patients aged 6 - 79 years, including pulmonary function (PF) data such as forced expiratory flow between 25% and 75% of forced vital capacity (FEF<sub>25-75</sub>), forced expiratory volume in 1 second (FEV<sub>1</sub>), forced expiratory volume in 3 seconds (FEV<sub>3</sub>), forced expiratory volume in 6 seconds (FEV<sub>6</sub>), and forced vital capacity (FVC). To evaluate the small airway function, we calculated z-scores for FEF<sub>25-75</sub>, FEF<sub>25-75</sub>/FVC, FEV<sub>1</sub>/FEV<sub>6</sub>, and FEV<sub>3</sub>/FEV<sub>6</sub>. Logistic regression determined the adjusted odds ratios (aORs) for symptoms and comorbidity.</p><p><strong>Results: </strong>FEF<sub>25-75</sub>, FEV<sub>1</sub>/FEV<sub>6</sub>, and FEV<sub>3</sub>/FEV<sub>6</sub> correlated with asthmatic symptoms. FEF<sub>25-75</sub> had the strongest association with wheezing or whistling attacks. An increase of 1 standard deviations (SD) in FEF<sub>25-75</sub> reduced recurrent wheezing (aOR: 0.70; 95% confidence intervals (95% CIs): 0.65 - 0.76) and severe attacks (aOR: 0.67; 95% CI: 0.62 - 0.94). These indices were also linked to dry cough and hay fever, particularly FEV<sub>3</sub>/FEV<sub>6</sub> reducing hay fever risk (aOR: 0.70; 95% CI: 0.55 - 0.91) in non-T2 asthma. FEF<sub>25-75</sub>/FVC related to persistent (aOR: 0.78; 95% CI: 0.72 - 0.84) and severe attacks (aOR: 1.14; 95% CI: 1.08 - 1.22) in non-T2 groups. Lower indices combined with T2 exposure raised severe attack risk.</p><p><strong>Conclusions: </strong>In this nationwide study, small airway function correlated with symptom onset, especially in T2 asthma. Small airway injury differed between T2 and non-T2 asthma. Prospective research is needed to establish reference values.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 5","pages":"220-231"},"PeriodicalIF":2.0000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11161183/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of Small Airway Functional Indices With Respiratory Symptoms and Comorbidity in Asthmatics: A National Cross-Sectional Study.\",\"authors\":\"Jia Wei Long, Yong Liang Jiang\",\"doi\":\"10.14740/jocmr5158\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Small airway dysfunction (SAD) and airway inflammation are vital in asthma exacerbations. Type 2 inflammation (T2), mediated by cytokines from T helper 2 cell (Th2) such as interleukin (IL)-4, IL-5, and IL-13, is a potential mechanism underlying SAD. Research on small airway function in asthma is limited. We aimed to explore the correlation between small airway function and respiratory symptoms and comorbidity in T2 and non-T2 asthma.</p><p><strong>Methods: </strong>Derived from the National Health and Nutrition Examination Survey (NHANES), our study encompassed 2,420 asthma patients aged 6 - 79 years, including pulmonary function (PF) data such as forced expiratory flow between 25% and 75% of forced vital capacity (FEF<sub>25-75</sub>), forced expiratory volume in 1 second (FEV<sub>1</sub>), forced expiratory volume in 3 seconds (FEV<sub>3</sub>), forced expiratory volume in 6 seconds (FEV<sub>6</sub>), and forced vital capacity (FVC). To evaluate the small airway function, we calculated z-scores for FEF<sub>25-75</sub>, FEF<sub>25-75</sub>/FVC, FEV<sub>1</sub>/FEV<sub>6</sub>, and FEV<sub>3</sub>/FEV<sub>6</sub>. Logistic regression determined the adjusted odds ratios (aORs) for symptoms and comorbidity.</p><p><strong>Results: </strong>FEF<sub>25-75</sub>, FEV<sub>1</sub>/FEV<sub>6</sub>, and FEV<sub>3</sub>/FEV<sub>6</sub> correlated with asthmatic symptoms. FEF<sub>25-75</sub> had the strongest association with wheezing or whistling attacks. An increase of 1 standard deviations (SD) in FEF<sub>25-75</sub> reduced recurrent wheezing (aOR: 0.70; 95% confidence intervals (95% CIs): 0.65 - 0.76) and severe attacks (aOR: 0.67; 95% CI: 0.62 - 0.94). These indices were also linked to dry cough and hay fever, particularly FEV<sub>3</sub>/FEV<sub>6</sub> reducing hay fever risk (aOR: 0.70; 95% CI: 0.55 - 0.91) in non-T2 asthma. FEF<sub>25-75</sub>/FVC related to persistent (aOR: 0.78; 95% CI: 0.72 - 0.84) and severe attacks (aOR: 1.14; 95% CI: 1.08 - 1.22) in non-T2 groups. Lower indices combined with T2 exposure raised severe attack risk.</p><p><strong>Conclusions: </strong>In this nationwide study, small airway function correlated with symptom onset, especially in T2 asthma. Small airway injury differed between T2 and non-T2 asthma. Prospective research is needed to establish reference values.</p>\",\"PeriodicalId\":94329,\"journal\":{\"name\":\"Journal of clinical medicine research\",\"volume\":\"16 5\",\"pages\":\"220-231\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11161183/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of clinical medicine research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr5158\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr5158","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Association of Small Airway Functional Indices With Respiratory Symptoms and Comorbidity in Asthmatics: A National Cross-Sectional Study.
Background: Small airway dysfunction (SAD) and airway inflammation are vital in asthma exacerbations. Type 2 inflammation (T2), mediated by cytokines from T helper 2 cell (Th2) such as interleukin (IL)-4, IL-5, and IL-13, is a potential mechanism underlying SAD. Research on small airway function in asthma is limited. We aimed to explore the correlation between small airway function and respiratory symptoms and comorbidity in T2 and non-T2 asthma.
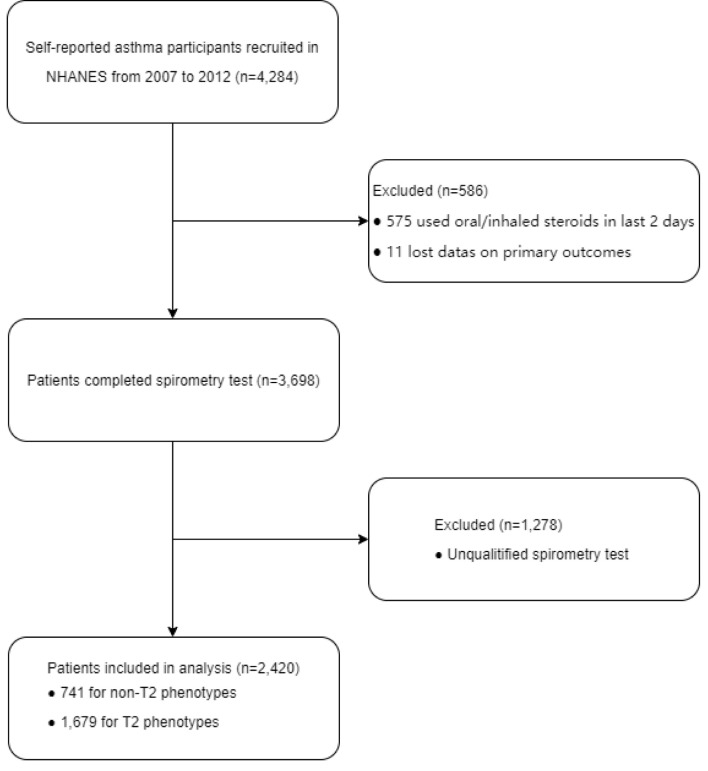
Methods: Derived from the National Health and Nutrition Examination Survey (NHANES), our study encompassed 2,420 asthma patients aged 6 - 79 years, including pulmonary function (PF) data such as forced expiratory flow between 25% and 75% of forced vital capacity (FEF25-75), forced expiratory volume in 1 second (FEV1), forced expiratory volume in 3 seconds (FEV3), forced expiratory volume in 6 seconds (FEV6), and forced vital capacity (FVC). To evaluate the small airway function, we calculated z-scores for FEF25-75, FEF25-75/FVC, FEV1/FEV6, and FEV3/FEV6. Logistic regression determined the adjusted odds ratios (aORs) for symptoms and comorbidity.
Results: FEF25-75, FEV1/FEV6, and FEV3/FEV6 correlated with asthmatic symptoms. FEF25-75 had the strongest association with wheezing or whistling attacks. An increase of 1 standard deviations (SD) in FEF25-75 reduced recurrent wheezing (aOR: 0.70; 95% confidence intervals (95% CIs): 0.65 - 0.76) and severe attacks (aOR: 0.67; 95% CI: 0.62 - 0.94). These indices were also linked to dry cough and hay fever, particularly FEV3/FEV6 reducing hay fever risk (aOR: 0.70; 95% CI: 0.55 - 0.91) in non-T2 asthma. FEF25-75/FVC related to persistent (aOR: 0.78; 95% CI: 0.72 - 0.84) and severe attacks (aOR: 1.14; 95% CI: 1.08 - 1.22) in non-T2 groups. Lower indices combined with T2 exposure raised severe attack risk.
Conclusions: In this nationwide study, small airway function correlated with symptom onset, especially in T2 asthma. Small airway injury differed between T2 and non-T2 asthma. Prospective research is needed to establish reference values.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


