{"title":"一例利用持续性 CAR-T 细胞成功治疗 DLBCL 早期孤立性中枢神经系统复发的病例。","authors":"Ken Takigawa, Noriaki Kawano, Yasuo Mori, Takuji Yamauchi, Taro Tochigi, Kohta Miyawaki, Kyohei Mori, Masatoshi Shimo, Takashi Nakaike, Kiyoshi Yamashita, Koichi Mashiba, Ikuo Kikuchi, Kousuke Marutsuka, Koichi Ohshima, Koji Kato, Koichi Akashi","doi":"10.31547/bct-2023-032","DOIUrl":null,"url":null,"abstract":"<p><p>Secondary central nervous system (CNS) lymphomas typically require CNS-penetrating drugs; however, the available agents are limited with temporary effects and poor outcomes. Chimeric antigen receptor T (CAR-T) cell therapy (lisocabtagene maraleucel; liso-cel) has been used to treat a few cases of isolated secondary CNS lymphoma. Herein, we report the case of a 66-year-old male diagnosed with diffuse large B-cell lymphoma (Ann Arbor grade IV; R-IPI, good risk; CNS IPI: Intermediate risk) who achieved complete remission (CR) after six courses of R-CHOP therapy. Three months later, he presented with ptosis and eye movement disorder. Systemic CT and bone marrow examination revealed no lymphoma. Although cranial-enhanced MRI showed normal findings, an increased number of B-cells (51/μL) with the original lymphoma phenotype (CD19+CD79a+CD5-CD10-CD20-Igλ+) was detected in cerebrospinal fluid (CSF), indicating an isolated CNS relapse. Seven high-dose methotrexate courses led to partial response. Subsequently, the patient received CAR-T cell therapy with tolerable adverse events - cytokine release syndrome treated with tocilizumab, no immune effector cell-associated neurotoxicity syndrome, and bone marrow failure treated with granulocyte-colony stimulating factor and eltrombopag. Sequential flow cytometry revealed a high peak of CAR-T cells and the presence of residual CAR-T cells in the peripheral blood, indicating immune surveillance of CNS lymphoma by CAR-T cells. This treatment led to a second CR. This case is the first to validate the efficacy and safety of CAR-T cell therapy for isolated secondary CNS lymphoma in clinical practice. Future accumulation of evidence on the efficacy and safety of CAR-T cell therapy is essential.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"7 2","pages":"37-40"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11153208/pdf/","citationCount":"0","resultStr":"{\"title\":\"A case of successful CAR-T cell therapy for early isolated CNS recurrence of DLBCL with persistent CAR-T cells.\",\"authors\":\"Ken Takigawa, Noriaki Kawano, Yasuo Mori, Takuji Yamauchi, Taro Tochigi, Kohta Miyawaki, Kyohei Mori, Masatoshi Shimo, Takashi Nakaike, Kiyoshi Yamashita, Koichi Mashiba, Ikuo Kikuchi, Kousuke Marutsuka, Koichi Ohshima, Koji Kato, Koichi Akashi\",\"doi\":\"10.31547/bct-2023-032\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Secondary central nervous system (CNS) lymphomas typically require CNS-penetrating drugs; however, the available agents are limited with temporary effects and poor outcomes. Chimeric antigen receptor T (CAR-T) cell therapy (lisocabtagene maraleucel; liso-cel) has been used to treat a few cases of isolated secondary CNS lymphoma. Herein, we report the case of a 66-year-old male diagnosed with diffuse large B-cell lymphoma (Ann Arbor grade IV; R-IPI, good risk; CNS IPI: Intermediate risk) who achieved complete remission (CR) after six courses of R-CHOP therapy. Three months later, he presented with ptosis and eye movement disorder. Systemic CT and bone marrow examination revealed no lymphoma. Although cranial-enhanced MRI showed normal findings, an increased number of B-cells (51/μL) with the original lymphoma phenotype (CD19+CD79a+CD5-CD10-CD20-Igλ+) was detected in cerebrospinal fluid (CSF), indicating an isolated CNS relapse. Seven high-dose methotrexate courses led to partial response. Subsequently, the patient received CAR-T cell therapy with tolerable adverse events - cytokine release syndrome treated with tocilizumab, no immune effector cell-associated neurotoxicity syndrome, and bone marrow failure treated with granulocyte-colony stimulating factor and eltrombopag. Sequential flow cytometry revealed a high peak of CAR-T cells and the presence of residual CAR-T cells in the peripheral blood, indicating immune surveillance of CNS lymphoma by CAR-T cells. This treatment led to a second CR. This case is the first to validate the efficacy and safety of CAR-T cell therapy for isolated secondary CNS lymphoma in clinical practice. Future accumulation of evidence on the efficacy and safety of CAR-T cell therapy is essential.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"7 2\",\"pages\":\"37-40\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-03-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11153208/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2023-032\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2023-032","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A case of successful CAR-T cell therapy for early isolated CNS recurrence of DLBCL with persistent CAR-T cells.
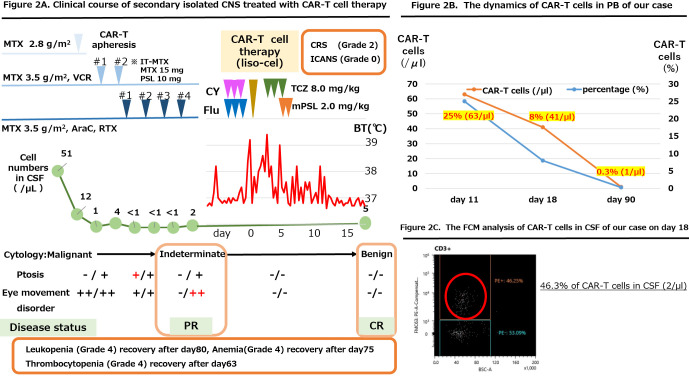
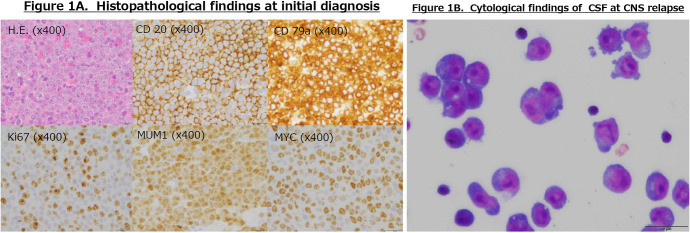
Secondary central nervous system (CNS) lymphomas typically require CNS-penetrating drugs; however, the available agents are limited with temporary effects and poor outcomes. Chimeric antigen receptor T (CAR-T) cell therapy (lisocabtagene maraleucel; liso-cel) has been used to treat a few cases of isolated secondary CNS lymphoma. Herein, we report the case of a 66-year-old male diagnosed with diffuse large B-cell lymphoma (Ann Arbor grade IV; R-IPI, good risk; CNS IPI: Intermediate risk) who achieved complete remission (CR) after six courses of R-CHOP therapy. Three months later, he presented with ptosis and eye movement disorder. Systemic CT and bone marrow examination revealed no lymphoma. Although cranial-enhanced MRI showed normal findings, an increased number of B-cells (51/μL) with the original lymphoma phenotype (CD19+CD79a+CD5-CD10-CD20-Igλ+) was detected in cerebrospinal fluid (CSF), indicating an isolated CNS relapse. Seven high-dose methotrexate courses led to partial response. Subsequently, the patient received CAR-T cell therapy with tolerable adverse events - cytokine release syndrome treated with tocilizumab, no immune effector cell-associated neurotoxicity syndrome, and bone marrow failure treated with granulocyte-colony stimulating factor and eltrombopag. Sequential flow cytometry revealed a high peak of CAR-T cells and the presence of residual CAR-T cells in the peripheral blood, indicating immune surveillance of CNS lymphoma by CAR-T cells. This treatment led to a second CR. This case is the first to validate the efficacy and safety of CAR-T cell therapy for isolated secondary CNS lymphoma in clinical practice. Future accumulation of evidence on the efficacy and safety of CAR-T cell therapy is essential.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


